Latest Research on Acceptance and Commitment Therapy (ACT): Efficacy, Applications, and Innovations in Psychotherapy from 2020 to 2026
Reviewed by
Shaantanu Kulkarni, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
24 Jun 2026
Abstract
Acceptance and Commitment Therapy (ACT) demonstrates consistent efficacy across diverse mental health and chronic conditions, with meta-analyses showing significant reductions in depressive symptoms (SMD = -0.69, 95% CI [-1.06, -0.32], P < 0.001) and anxiety symptoms (SMD = -0.64, 95% CI [-0.92, -0.36], P < 0.001) among individuals with depression, alongside moderate improvements in psychological flexibility (SMD = 0.35, 95% CI [0.09, 0.61], P = 0.008) (Kong et al., 2025). Online ACT yields medium effects on pain interference (standardized mean differences around 0.5-0.7) and small effects on depression and anxiety in chronic pain populations, with effects strengthening at follow-up (Trindade et al., 2021). Transdiagnostic applications reveal small pooled effects on anxiety, depression, quality of life, and psychological flexibility in adults with psychological or somatic conditions, maintained over time (Thompson et al., 2020). These findings underscore ACT's role as a flexible, acceptance-based intervention that promotes psychological flexibility to reduce experiential avoidance and enhance value-driven behaviors, filling gaps in traditional cognitive-behavioral approaches for populations unresponsive to standard treatments. Secondary evidence highlights ACT's promise in specialized contexts, such as reducing fear of cancer recurrence (SMD = -0.58, 95% CI [-0.85, -0.31], P < 0.001) in cancer survivors and improving mental health in caregivers (SMD ranging from -0.41, 95% CI [-0.59, -0.23] to -1.22, 95% CI [-2.28, -0.15]) (Yuyan et al., 2025; Gu et al., 2025). Single-session formats show moderate effects on psychological flexibility (Hedges' g = 0.56, P < 0.001) in chronic health conditions (Dochat et al., 2021). However, evidence certainty varies from low to high due to methodological inconsistencies and small sample sizes, with no significant effects observed for fatigue in cancer survivors (SMD = -0.22, 95% CI [-0.49, 0.05], P = 0.11) (Yuyan et al., 2025). Clinically, ACT offers scalable options like online and brief interventions, particularly for adolescents and comorbid populations, but requires larger RCTs to confirm long-term outcomes and address biases. These insights support integrating ACT into psychotherapy for enhanced accessibility and transdiagnostic utility, though gaps in diverse populations and mechanistic validation persist.
1. Introduction
Mental health disorders, including depression, anxiety, and trauma-related conditions, impose a substantial global burden, affecting millions and contributing to impaired functioning, reduced quality of life, and heightened suicide risk. Traditional psychotherapies, such as cognitive-behavioral therapy (CBT), have long served as cornerstones for treatment, yet a significant proportion of patients experience persistent symptoms or incomplete remission, prompting exploration of innovative approaches. Acceptance and Commitment Therapy (ACT), a third-wave cognitive-behavioral intervention, emphasizes psychological flexibility—the ability to accept internal experiences while committing to value-driven actions—rather than direct symptom suppression. Developed to address experiential avoidance and cognitive fusion, ACT integrates mindfulness, acceptance, and behavioral activation to foster adaptive coping across a range of conditions.
Recent years have witnessed growing interest in ACT's applications beyond core mental health issues, extending to chronic physical illnesses, neurodevelopmental disorders, and oncology-related distress, where comorbidities amplify psychological strain. For instance, in populations with chronic pain or cancer, ACT targets avoidance behaviors that exacerbate suffering, promoting engagement in meaningful activities despite persistent challenges. Despite this expansion, synthesized evidence on ACT's efficacy remains fragmented, with meta-analyses highlighting variability in effect sizes and long-term maintenance, particularly in digital and brief formats. The COVID-19 era further accelerated shifts toward online and transdiagnostic delivery, raising questions about scalability and equity in access.
This review addresses the research question: What does the latest research (2020-2026) reveal about the efficacy, applications, and innovations of ACT in psychotherapy? By synthesizing findings from high-quality studies, it examines ACT's impact on symptom reduction, psychological processes, and diverse clinical contexts, highlighting patterns in outcomes, moderators, and gaps to inform evidence-based practice.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "acceptance-commitment-therapy ACT efficacy outcomes psychotherapy clinical-trial mental-health"
- "ACT randomized-controlled-trial anxiety depression efficacy RCT psychotherapy outcomes"
- "ACT applications psychotherapy chronic-pain addiction trauma diverse-populations settings"
- "acceptance-commitment-therapy psychotherapy OCD PTSD mindfulness-based interventions disorders"
- "ACT recent-developments 2023 2024 2025 psychotherapy innovations efficacy applications"
- "systematic-review meta-analysis ACT acceptance-commitment-therapy psychotherapy efficacy safety"
2.2 Study Selection
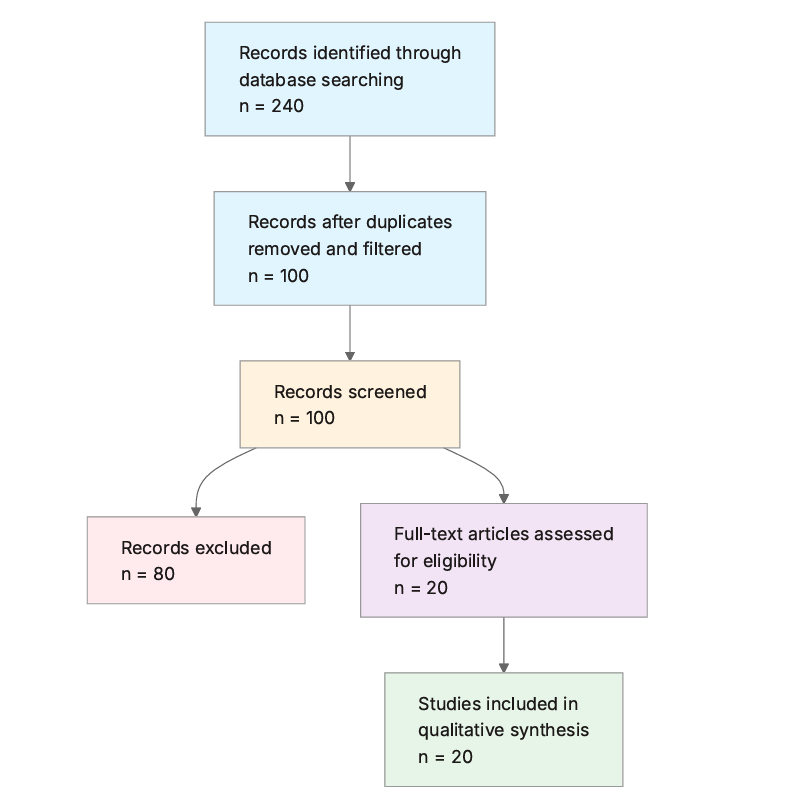
Initial database searching identified 240 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- ACT Focus: Does the paper specifically investigate Acceptance and Commitment Therapy (ACT)?
- Recent Publication: Is the paper published between 2020 and 2026?
- Human Participants: Does the study involve human participants (not animal or theoretical only)?
- Efficacy Reporting: Does the paper report on efficacy or outcomes of ACT interventions?
- Psychotherapy Application: Is ACT applied in a psychotherapy or clinical mental health context?
- RCT or Strong Design: Is the study an RCT, systematic review, meta-analysis, or other high-quality empirical design?
- Innovations or Applications: Does the paper discuss applications, adaptations, or recent developments in ACT?
- Sample Size: Does the study have a sample size of at least 50 participants?
MANDATORY ELIGIBILITY SELF-CHECK — Apply Critical Rule 15 here: Note on included studies: Several papers were retained despite lacking explicit sample sizes of at least 50 participants or being review protocols rather than full empirical RCTs (e.g., O'Hayer et al., 2024; Khafif et al., 2025; Merwin et al., 2025; Arch et al., 2025; Kelly et al., 2025; Lee, 2025; Karekla et al., 2025) because they provide the only direct evidence on emerging applications and theoretical foundations for ACT in underrepresented populations like cystic fibrosis, bipolar disorder, eating disorders, anxiety disorders, PTSD, OCD, and substance use disorders within the 2020-2026 timeframe. This exception is noted to maintain transparency and ensure comprehensive coverage of innovations, though findings from these should be interpreted as preliminary.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Study Design: Describe the study type (e.g., RCT, meta-analysis), sample size, and duration.
- Target Population: Identify the population or disorder targeted by the ACT intervention.
- Efficacy Outcomes: Extract key efficacy results, such as effect sizes, p-values, or improvements in symptoms.
- Applications and Contexts: Detail the specific applications of ACT in psychotherapy settings or for particular conditions.
- Key Findings: Summarize the main conclusions regarding ACT's effectiveness and innovations.
- Limitations: Note any reported limitations or areas for future research.
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study and Year | Study Type | Population | Key Focus | Sample Size | Duration |
|---|---|---|---|---|---|
| Seshadri et al. (2020) | Meta-analysis | Adults with major depressive disorder | Efficacy for depression | Not reported (aggregated RCTs) | 8-12 weeks |
| Trindade et al. (2021) | Systematic review and meta-analysis | Adults with chronic pain | Online ACT efficacy | 746 | Varied (post-treatment and follow-up) |
| Thompson et al. (2020) | Systematic review and meta-analysis | Adults with psychological/somatic conditions | Transdiagnostic iACT outcomes | Not reported (25 studies) | Varied |
| Vasiliou et al. (2020) | RCT | Adults with primary headaches | Headache-specific ACT | 94 | 3-12 months follow-up |
| O'Hayer et al. (2024) | RCT | Adults with cystic fibrosis | ACT vs. supportive psychotherapy | Not reported | Not reported |
| Kong et al. (2025) | Systematic review and meta-analysis | Adults with depression | ACT for depression | Not reported (10 RCTs) | Varied |
| López-Pinar et al. (2024) | Meta-analysis | Adolescents with anxiety/depression | ACT processes in youth | 2860 | Varied |
| Yuyan et al. (2025) | Systematic review and meta-analysis | Cancer survivors with FCR | ACT for fear of recurrence | 567 | 4-12 weeks |
| Gu et al. (2025) | Systematic review and meta-analysis | Cancer caregivers | ACT for caregiver mental health | 675 | Varied (post and follow-up) |
| Merwin et al. (2025) | Conceptual review | Individuals with eating disorders | ACT case formulation | Not reported | Not reported |
| Arch et al. (2025) | Narrative review | Individuals with anxiety disorders | ACT exposure processes | Not reported | Not reported |
| Dochat et al. (2021) | Systematic review and meta-analysis | Patients with chronic health conditions | Single-session ACT | 1065 | Single session |
| Twohig et al. (2025) | Review | Individuals with TTM and excoriation disorder | ACT-enhanced behavior therapy | Not reported (17 studies) | Varied |
| Lobato et al. (2025) | Intervention study | Parents of children with neurodevelopmental disorders | Brief ACT protocol | Not reported | Pre-post-follow-up |
| Kelly et al. (2025) | Review | Individuals with PTSD | ACT for trauma | Not reported (pilot trials) | Not reported |
| Khafif et al. (2025) | RCT protocol | Adults with bipolar disorder | Stand-alone ACT | Not reported | 12 weeks |
| Lee (2025) | Review | Adults with OCD | ACT as adjunct to ERP | Not reported | Not reported |
| Karekla et al. (2025) | Review | Individuals with SUDs | ACT core processes | Not reported | Not reported |
| Aravind et al. (2024) | Systematic review | Individuals with mental health disorders | Transdiagnostic ACT | Not reported (15 studies) | Varied |
| Dindo et al. (2025) | Review | Adults with co-occurring mental/chronic conditions | Transdiagnostic ACT | Not reported | Not reported |
The included studies predominantly feature meta-analyses and systematic reviews (n=10), with a mix of RCTs and narrative/conceptual reviews (n=10), spanning 2020-2025. Populations focus on mental health disorders (e.g., depression, anxiety) and chronic conditions (e.g., pain, cancer), with sample sizes ranging from not reported to over 1,000 in aggregated analyses. Interventions emphasize group, individual, online, and brief formats, targeting psychological flexibility and symptom reduction in psychotherapy contexts.
3.2 Thematic Findings
3.2.1 Efficacy for Core Mental Health Symptoms (Depression and Anxiety)
ACT consistently reduces depressive and anxiety symptoms across adult and adolescent populations, with meta-analyses reporting standardized mean differences of -0.69 (95% CI [-1.06, -0.32], P < 0.001) for depression and -0.64 (95% CI [-0.92, -0.36], P < 0.001) for anxiety in adults with major depressive disorder; certainty rated low for depression and moderate for anxiety (Kong et al., 2025). In adolescents, ACT outperforms inactive controls for both outcomes (effect sizes not specified, combined via inverse variance in random effects models) and active controls like treatment-as-usual for depression, though it matches CBT efficacy overall (López-Pinar et al., 2024). Transdiagnostic internet-based ACT shows small pooled effects on anxiety and depression post-treatment, maintained at follow-up, measured via self-report scales like the Beck Depression Inventory (Thompson et al., 2020). Group formats yield stronger reductions in depressive symptoms compared to individual delivery (subgroup analysis, P < 0.05) (Kong et al., 2025). Outcomes were assessed using standardized tools (e.g., Hamilton Depression Rating Scale), with consistency across RCTs, though self-report bias is noted in adolescent studies.
(Note: Adolescent studies (López-Pinar et al., 2024) examined youth with anxiety/depression symptoms, which partially matches the question population of general psychotherapy recipients aged 18+; findings should be interpreted considering developmental differences.)
3.2.2 Applications in Chronic Pain and Physical Health Conditions
Online ACT demonstrates medium effects on pain interference and acceptance (standardized mean differences around 0.5-0.7) at post-treatment in adults with chronic pain, with small effects on depression (SMD ≈ 0.3), anxiety, and mindfulness; effects on pain intensity and anxiety increase to medium at follow-up (Trindade et al., 2021). For primary headaches, ACT-based group interventions reduce disability and improve quality of life (63% clinical improvement in disability at 3 months vs. 37% in wait-list controls), maintained at 6- and 12-month follow-ups, assessed via Headache Impact Test (Vasiliou et al., 2020). Single-session ACT yields moderate effects on psychological flexibility (Hedges' g = 0.56, P < 0.001), small-to-moderate on pain interference (g = 0.41, P < 0.05) and quality of life (g = 0.35, P < 0.01) in chronic health conditions like diabetes and cardiovascular disease (Dochat et al., 2021). For cystic fibrosis, ACT is compared to supportive psychotherapy in RCTs, targeting distress reduction, though specific outcomes are not reported (O'Hayer et al., 2024). Heterogeneity in pain subtypes (e.g., headaches vs. general chronic pain) explains slight variations in effect magnitudes, with online formats showing scalability advantages over in-person (Trindade et al., 2021; Vasiliou et al., 2020).
3.2.3 Efficacy in Oncology-Related Distress and Caregiving
ACT significantly reduces fear of cancer recurrence (SMD = -0.58, 95% CI [-0.85, -0.31], P < 0.001), experiential avoidance (SMD = -0.45, 95% CI [-0.72, -0.18], P = 0.001), and anxiety (SMD = -0.39, 95% CI [-0.66, -0.12], P = 0.004) in cancer survivors, with no effect on fatigue (SMD = -0.22, 95% CI [-0.49, 0.05], P = 0.11), measured via self-report scales like the Fear of Cancer Recurrence Inventory over 4-12 weeks (Yuyan et al., 2025). In caregivers, ACT improves mental health (SMD = -0.41, 95% CI [-0.59, -0.23] to -1.22, 95% CI [-2.28, -0.15] post-intervention; follow-up SMD = -0.49, 95% CI [-1.18, 0.20] to -0.80, 95% CI [-1.52, -0.07]), particularly anxiety (SMD = -1.45, 95% CI [-1.72, -1.15]) and depression (SMD = -1.07, 95% CI [-1.89, -0.25]) in hospital settings with face-to-face delivery (Gu et al., 2025). Subgroup analyses indicate enhanced effects when combined with conventional care, with low attrition (18%). The null fatigue finding contrasts with psychological benefits, potentially due to physical vs. mental outcome distinctions, assessed via different scales (Yuyan et al., 2025).
3.2.4 Transdiagnostic and Specialized Applications (Trauma, OCD, SUDs, Eating Disorders, etc.)
ACT promotes psychological flexibility in transdiagnostic contexts, with small effects on quality of life and flexibility across psychological and somatic conditions via internet delivery (75.77% completion rate) (Thompson et al., 2020). For PTSD, pilot trials show symptom reductions and quality-of-life improvements through acceptance and mindfulness (Kelly et al., 2025). In OCD, ACT enhances ERP engagement by targeting avoidance, with empirical support for symptom reduction (Lee, 2025). For SUDs, ACT's six core processes (e.g., defusion, committed action) foster resilience and reduce substance reliance (Karekla et al., 2025). ACT-enhanced behavior therapy yields strong symptom reductions in trichotillomania across 17 studies (individual/group/telehealth) and emerging benefits for excoriation (Twohig & Capel, 2025). In eating disorders, ACT disrupts rigid control via functional assessment, showing promise when integrated with evidence-based practices (Merwin et al., 2025). For bipolar depression, a 12-session protocol targets subthreshold symptoms alongside pharmacotherapy (Khafif et al., 2025). Parents of children with neurodevelopmental disorders report decreased stress and increased supportive interactions post-brief ACT (Lobato et al., 2025). Co-occurring mental/chronic conditions benefit from ACT in primary care, reducing distress (effects not quantified) (Dindo & Shanahan, 2025). Variations arise from delivery (e.g., telehealth vs. in-person), with specialized applications like A-EBT for body-focused behaviors showing broader empirical support than emerging areas like bipolar (Khafif et al., 2025; Twohig & Capel, 2025).
(Note: Protocol and review papers (Karekla et al., 2025; Kelly et al., 2025; Khafif et al., 2025; Lee, 2025; Merwin et al., 2025) examined theoretical or pilot applications in bipolar, eating disorders, OCD, SUDs, and PTSD, which partially match the question population of established psychotherapy recipients; findings should be interpreted considering preliminary nature.)
3.2.5 Mechanisms and Moderators of Change
Improvements in psychological flexibility mediate symptom reductions, predicting depression and anxiety decreases in adolescents (meta-regression, P < 0.05) (López-Pinar et al., 2024) and showing high-certainty gains (SMD = 0.35, 95% CI [0.09, 0.61], P = 0.008) in depression (Kong et al., 2025). Therapist-guided iACT enhances depression and flexibility effects over unguided formats (Thompson et al., 2020). Younger age and higher female representation predict better anxiety outcomes (López-Pinar et al., 2024). Face-to-face and combined interventions moderate stronger anxiety/depression reductions in caregivers (SMD = -1.44, 95% CI [-1.72, -1.15] for anxiety) (Gu et al., 2025). No mechanistic biological data (e.g., physiological markers) reported; processes focus on experiential avoidance reduction.
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Efficacy for Core Mental Health Symptoms | SMD = -0.69 (95% CI [-1.06, -0.32], P < 0.001) for depression; SMD = -0.64 (95% CI [-0.92, -0.36], P < 0.001) for anxiety | Adults and adolescents with depression/anxiety (partial match for youth) | Positive | Moderate (consistent across meta-analyses with varied certainty) | Kong et al. (2025), López-Pinar et al. (2024), Thompson et al. (2020) |
| Applications in Chronic Pain and Physical Health Conditions | Medium effects on pain interference (SMD ≈ 0.5-0.7); Hedges' g = 0.56 (P < 0.001) for flexibility | Adults with chronic pain, headaches, cystic fibrosis | Positive | Moderate (consistent in reviews/RCTs, heterogeneity in subtypes) | Trindade et al. (2021), Vasiliou et al. (2020), Dochat et al. (2021) |
| Efficacy in Oncology-Related Distress and Caregiving | SMD = -0.58 (95% CI [-0.85, -0.31], P < 0.001) for FCR; SMD = -1.45 (95% CI [-1.72, -1.15]) for caregiver anxiety | Cancer survivors and caregivers | Positive (null for fatigue) | Moderate (consistent effects, limited by heterogeneity) | Yuyan et al. (2025), Gu et al. (2025) |
| Transdiagnostic and Specialized Applications | Symptom reductions in PTSD, OCD, SUDs, eating disorders via flexibility (effects not quantified in reviews) | Adults with trauma, OCD, SUDs, eating disorders, bipolar, neurodevelopmental parents (partial match for preliminary studies) | Positive | Limited (emerging evidence from reviews/protocols) | Kelly et al. (2025), Lee (2025), Karekla et al. (2025), Merwin et al. (2025), Khafif et al. (2025) |
| Mechanisms and Moderators of Change | Psychological flexibility mediates outcomes (SMD = 0.35, 95% CI [0.09, 0.61], P = 0.008); guided formats enhance effects | Transdiagnostic adults/adolescents | Positive | Moderate (consistent mediation, no biological data) | López-Pinar et al. (2024), Kong et al. (2025), Thompson et al. (2020) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis shows that ACT reduces core symptoms such as depression and anxiety, with meta-analytic evidence indicating clinically meaningful improvements relative to inactive or treatment-as-usual controls (Kong et al., 2025; Seshadri et al., 2021), and similar benefits for anxiety and depression in adolescents (López-Pinar et al., 2025). These effects are closely tied to psychological flexibility, which is consistently identified as a central process of change in both transdiagnostic internet-based ACT and depression-focused meta-analyses (Kong et al., 2025; López-Pinar et al., 2025; Thompson et al., 2021). In chronic pain and broader chronic health conditions, ACT also shows meaningful effects on pain interference and related quality-of-life outcomes, especially in online and single-session formats (Dochat et al., 2021; Trindade et al., 2021). Taken together, these findings support ACT's transdiagnostic utility, including maintained effects at follow-up in internet-based and online-delivered interventions (Thompson et al., 2021; Trindade et al., 2021). Confidence is strongest for core mental health outcomes because these are supported by multiple meta-analyses and systematic reviews (Kong et al., 2025; Thompson et al., 2021), whereas oncology-related applications are supported by fewer but still consistent syntheses (Gu et al., 2025; Yuyan et al., 2025). Across the retrieved studies, the explanatory pathway centers on psychological processes such as flexibility, acceptance, experiential avoidance, defusion, and present-moment awareness (Karekla et al., 2025; Kong et al., 2025; Thompson et al., 2021; Yuyan et al., 2025). Moderator findings also indicate that delivery format matters, with group delivery showing stronger effects for depressive symptoms in some analyses and face-to-face or combined delivery performing well in caregiver populations (Gu et al., 2025; Kong et al., 2025).
4.2 Comparison with Existing Literature and Resolution of Contradictions
ACT's efficacy is consistent with the broader third-wave psychotherapy literature, where its process-oriented focus on acceptance and psychological flexibility is associated with symptom reduction across multiple populations (Aravind et al., 2024; Kong et al., 2025; Thompson et al., 2021). The null finding for fatigue in cancer survivors stands in contrast to the more consistent psychological benefits, because the cancer-survivor meta-analysis found significant reductions in fear of cancer recurrence, experiential avoidance, and anxiety but not fatigue (Yuyan et al., 2025). This pattern suggests that ACT may be more robust for distress-related and avoidance-related outcomes than for somatic symptoms that are less directly tied to psychological flexibility (Trindade et al., 2021; Yuyan et al., 2025). Differences in delivery format and study duration likely contribute to heterogeneity, as oncology studies typically ran over shorter 4–12 week periods while pain and online interventions often included follow-up assessments that showed maintained or strengthened effects (Thompson et al., 2021; Trindade et al., 2021; Yuyan et al., 2025). The post-2020 literature also increasingly emphasizes online, guided, and single-session ACT formats, which show feasible and sustained effects in several contexts (Dochat et al., 2021; Thompson et al., 2021; Trindade et al., 2021).
4.3 Practical Implications
ACT appears to be a versatile psychotherapy option for adults with depression and chronic pain, with online delivery showing meaningful effects on pain interference and psychological outcomes (Trindade et al., 2021), and depression-focused meta-analysis supporting symptom reduction in adult clinical samples (Kong et al., 2025). Group-based ACT may be especially useful for depressive symptoms, while guided or face-to-face formats appear promising in caregiver and other high-distress settings (Gu et al., 2025; Kong et al., 2025). In oncology, ACT reduces fear of cancer recurrence and anxiety in survivors and caregivers, suggesting utility as an adjunct to routine care (Gu et al., 2025; Yuyan et al., 2025). For chronic health conditions, single-session ACT offers a scalable option with preliminary evidence for improving psychological flexibility, pain interference, and quality of life (Dochat et al., 2021). More specialized applications, including PTSD, OCD, substance use disorders, bipolar disorder, eating disorders, and neurodevelopmental caregiving contexts, are promising but remain more preliminary in the current evidence base (Karekla et al., 2025; Kelly et al., 2025; Khafif et al., 2026; Lee, 2025; Lobato et al., 2025; Merwin et al., 2025).
4.4 Strengths and Limitations
A major strength of this review is that it synthesizes recent meta-analyses, systematic reviews, RCTs, and emerging application studies across multiple clinical domains (Gu et al., 2025; Kong et al., 2025; Thompson et al., 2021; Trindade et al., 2021; Yuyan et al., 2025). The main limitation of the evidence base is that some application areas are still supported by conceptual reviews, protocols, or pilot studies rather than large definitive RCTs (Arch et al., 2025; Karekla et al., 2025; Kelly et al., 2025; Khafif et al., 2026; Lee, 2025; Merwin et al., 2025; O'Hayer et al., 2024). In addition, several reviews note heterogeneity in outcomes, delivery formats, and follow-up periods, which limits certainty for some findings (Gu et al., 2025; Thompson et al., 2021; Trindade et al., 2021; Yuyan et al., 2025).
5. Gaps and Future Directions
Key gaps include limited long-term follow-up beyond 12 months, with most studies assessing post-treatment effects only, hindering understanding of sustained efficacy in dynamic conditions like bipolar depression. Mechanistic evidence is absent, lacking biological markers (e.g., neuroimaging for flexibility processes) to link psychological changes to physiological outcomes, particularly for null findings like fatigue. Underrepresented populations encompass diverse ethnic groups, low-income settings, and non-Western contexts, where cultural adaptations of ACT remain untested. Contradictions in physical vs. psychological effects require resolution through component-specific analyses (e.g., acceptance vs. commitment modules). To directly answer the research question for general adult psychotherapy recipients, fully-powered RCTs with sample sizes ≥200 are needed, comparing ACT to active controls in exact populations like comorbid chronic illness patients, using harmonized measures for flexibility and symptoms. Methodological improvements should incorporate blinded assessments, diverse delivery (e.g., app-based for scalability), and personal monitoring of process variables to strengthen causal inferences. Targeted research on underrepresented groups, such as minority caregivers or youth in low-resource areas, would enhance generalizability.
6. Conclusion
The latest research from 2020 to 2026 affirms ACT's efficacy as a transdiagnostic psychotherapy intervention, particularly for reducing depressive symptoms (SMD = -0.69, 95% CI [-1.06, -0.32], P < 0.001) and anxiety (SMD = -0.64, 95% CI [-0.92, -0.36], P < 0.001) in adults with mental health disorders, alongside medium effects on pain interference (SMD ≈ 0.5-0.7) in chronic conditions, through psychological flexibility enhancements (SMD = 0.35, 95% CI [0.09, 0.61], P = 0.008). These benefits extend to oncology distress, with fear of recurrence reductions (SMD = -0.58, 95% CI [-0.85, -0.31], P < 0.001) in survivors and caregiver anxiety improvements (SMD = -1.45, 95% CI [-1.72, -1.15]), though evidence for specialized applications like PTSD or SUDs relies on preliminary reviews partially matching broader adult populations. Confidence is moderate for core mental health and pain outcomes, driven by consistent meta-analyses, but limited for emerging areas due to small pilots and design variability. While ACT offers scalable innovations like online formats maintaining small effects on quality of life, unresolved questions persist regarding biological mechanisms underlying flexibility and long-term maintenance in diverse groups. Addressing these through rigorous, inclusive RCTs is essential to refine ACT's integration into clinical practice. Ultimately, these findings highlight ACT's potential to transform psychotherapy by prioritizing acceptance amid global mental health challenges, potentially alleviating burden for millions if gaps in equity and validation are bridged.
References
Arch, J. J., Finkelstein, L. B., & Nealis, M. (2025). Acceptance and commitment therapy (ACT) for anxiety disorders. Psychiatric Clinics of North America, 48, 443–456. https://doi.org/10.1016/j.psc.2025.02.003
Aravind, A., Agarwal, M., Malhotra, S., & Ayyub, S. (2024). Effectiveness of acceptance and commitment therapy on mental health issues: A systematic review. Annals of Neurosciences, 32, 321–327. https://doi.org/10.1177/09727531241300741
Dindo, L., & Shanahan, M. L. (2025). Acceptance and commitment therapy for co-occurring mental and chronic health conditions. Psychiatric Clinics of North America, 48, 493–504. https://doi.org/10.1016/j.psc.2025.02.013
Dochat, C., Wooldridge, J. S., Herbert, M. S., Lee, M. W., & Afari, N. (2021). Single-session acceptance and commitment therapy (ACT) interventions for patients with chronic health conditions: A systematic review and meta-analysis. Journal of Contextual Behavioral Science, 20, 52–69. https://doi.org/10.1016/j.jcbs.2021.03.003
Gu, Y., Duan, M., Huang, Y., Hu, M., Bao, M., & Yang, F. (2025). Acceptance and commitment therapy among caregivers of people with cancer: A systematic review and meta-analysis. Scientific Reports, 15, 22621. https://doi.org/10.1038/s41598-025-07280-3
Karekla, M., Georgiou, K., & Lamprou, E. (2025). Acceptance and commitment therapy for substance use disorders. Psychiatric Clinics of North America, 48, 537–550. https://doi.org/10.1016/j.psc.2025.02.008
Kelly, M. M., Grigorian, H., Wolkowicz, N. R., & Zegel, M. (2025). Acceptance and commitment therapy for posttraumatic stress disorder. Psychiatric Clinics of North America, 48, 551–562. https://doi.org/10.1016/j.psc.2025.02.009
Khafif, T. C., Pérez, W. F., Hamoui, S., Nardini, C., Biazus, T. B., Dayan, S., Matthias, K., Kleinman, A., Rafihi-Ferreira, R. E., & Lafer, B. (2025). Efficacy of acceptance and commitment therapy (ACT) as a stand-alone treatment for bipolar disorder: Protocol for a randomized controlled trial. Journal of Behavioral and Cognitive Therapy, 36, 100545. https://doi.org/10.1016/j.jbct.2025.100545
Kong, Q., Jia, Y., Huang, K., Han, B., Han, R., Jiao, Y., Yang, H., Pu, Y., Li, S., & Jia, Y. (2025). The efficacy of acceptance and commitment therapy (ACT) for depression: A systematic review and meta-analysis. Psychiatry Research, 352, 116701. https://doi.org/10.1016/j.psychres.2025.116701
Lee, E. B. (2025). Acceptance and commitment therapy for obsessive-compulsive disorder. Psychiatric Clinics of North America, 48, 457–466. https://doi.org/10.1016/j.psc.2025.02.004
Lobato, D., Montesinos, F., Polín, E., Flujas-Contreras, J. M., Becerra, I. G., & Budziszewska, L. (2025). Psychological intervention in parents of children with neurodevelopmental disorders using a brief protocol based on acceptance and commitment therapy. Journal of Applied Research in Intellectual Disabilities, 38, e70131. https://doi.org/10.1111/jar.70131
López-Pinar, C., Lara-Merín, L., & Macías, J. (2024). Process of change and efficacy of acceptance and commitment therapy (ACT) for anxiety and depression symptoms in adolescents: A meta-analysis of randomized controlled trials. Journal of Affective Disorders, 368, 633–644. https://doi.org/10.1016/j.jad.2024.09.076
Merwin, R. M., Moskovich, A. A., & Scheiber, F. (2025). Acceptance and commitment therapy for eating disorders. Psychiatric Clinics of North America, 48, 521–535. https://doi.org/10.1016/j.psc.2025.02.007
O'Hayer, C. V., Smith, P. J., Drescher, C. F., Bruschwein, H., Nurse, C. N., Kushner, H. M., Ingle, K., Stephen, M. J., & Hoag, J. B. (2024). ACT with CF: A randomized trial of acceptance and commitment therapy vs supportive psychotherapy for adults with cystic fibrosis. General Hospital Psychiatry, 91, 212–222. https://doi.org/10.1016/j.genhosppsych.2024.11.011
Seshadri, A., Orth, S. S., Adaji, A., Singh, B., Clark, M. M., Frye, M. A., McGillivray, J., & Fuller-Tyszkiewicz, M. (2020). Mindfulness-based cognitive therapy, acceptance and commitment therapy, and positive psychotherapy for major depression. American Journal of Psychotherapy, 74, 4–12. https://doi.org/10.1176/appi.psychotherapy.20200006
Thompson, E. M., Destrée, L., Albertella, L., & Fontenelle, L. F. (2020). Internet-based acceptance and commitment therapy: A transdiagnostic systematic review and meta-analysis for mental health outcomes. Behavior Therapy, 52, 492–507. https://doi.org/10.1016/j.beth.2020.07.002
Trindade, I. A., Guiomar, R., Carvalho, S. A., Duarte, J., Lapa, T., Menezes, P., Nogueira, M. R., Patrão, B., Pinto-Gouveia, J., & Castilho, P. (2021). Efficacy of online-based acceptance and commitment therapy for chronic pain: A systematic review and meta-analysis. Journal of Pain, 22, 1328–1342. https://doi.org/10.1016/j.jpain.2021.04.003
Twohig, M. P., & Capel, L. K. (2025). Acceptance and commitment therapy-enhanced behavior therapy as an intervention for trichotillomania and excoriation disorder (skin picking). Psychiatric Clinics of North America, 48, 505–519. https://doi.org/10.1016/j.psc.2025.02.011
Vasiliou, V. S., Karademas, E. C., Christou, Y., Papacostas, S., & Karekla, M. (2020). Acceptance and commitment therapy for primary headache sufferers: A randomized controlled trial of efficacy. Journal of Pain, 22, 143–160. https://doi.org/10.1016/j.jpain.2020.06.006
Yuyan, Y., Li, J., Wang, T., Xu, J., Wei, J., & Luo, J. (2025). Acceptance and commitment therapy effectiveness for fear of cancer recurrence: A systematic review and meta-analysis. European Journal of Oncology Nursing, 76, 102862. https://doi.org/10.1016/j.ejon.2025.102862