Latest Research on Bipolar Disorder Treatment: Evidence on Medications, Mood Stabilizers, Therapies, and Psychiatric Advances
Reviewed by
Shaantanu Kulkarni, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
23 Jun 2026
Abstract
Recent research on bipolar disorder treatment underscores the enduring efficacy of mood stabilizers like lithium and valproate for maintenance therapy, with lithium demonstrating superior relapse prevention compared to placebo (odds ratio 0.42, 95% CI 0.30-0.60, p<0.0001) and comparable outcomes to antipsychotics such as quetiapine and olanzapine (OR 0.96, 95% CI 0.66-1.40, p=0.84) in long-term studies averaging 29.1 months. Adjunctive atypical antipsychotics, including lurasidone and lumateperone, enhance remission rates in bipolar depression when added to mood stabilizers (RR 1.23, 95% CI 1.01-1.50, p=0.04), while psychosocial interventions like psychoeducational family therapy reduce relapses and hospitalizations over five years. Bright light therapy shows potential for depressive symptoms (SMD -0.69, 95% CI -1.20 to -0.18, p<0.01 in sensitivity analyses), though overall evidence is mixed due to heterogeneity. Bipolar disorder, characterized by recurrent manic and depressive episodes, imposes substantial disability and healthcare burden, yet treatment gaps persist in acute phases and special populations like youths and reproductive-age adults. This review synthesizes findings across pharmacological and non-pharmacological modalities, highlighting trends toward adjunctive strategies and personalized approaches informed by clinical correlates such as family history and episode patterns. Key secondary insights include lamotrigine's role in preventing depressive relapses (strongest evidence in maintenance) and declining lithium prescription rates in Western regions (from 27.7% pre-2010 to 17.1% post-2010), contrasted with stability in Asia. These patterns suggest a shift toward antipsychotics amid safety concerns like metabolic risks with olanzapine and quetiapine. Clinically, shared decision-making is essential for adjunctive therapies, balancing benefits like improved quality of life (SMD 0.22, 95% CI 0.06-0.37, p=0.005) against risks such as akathisia with cariprazine. Gaps remain in pediatric and geriatric applications, underscoring the need for targeted trials to refine 2026 psychiatric research priorities.
1. Introduction
Bipolar disorder is a chronic psychiatric condition marked by alternating episodes of mania or hypomania and depression, often interspersed with periods of euthymia, leading to profound disruptions in personal, social, and occupational functioning. Affecting approximately 1-2% of the global population, it ranks among the leading causes of disability worldwide, with high rates of relapse, hospitalization, and suicide that strain healthcare systems and impose significant economic burdens (Sajatovic, 2005). Effective management requires a multifaceted approach, combining pharmacotherapy to stabilize mood and prevent recurrences with psychosocial interventions to enhance adherence and coping. Mood stabilizers such as lithium and valproate have long served as cornerstones, particularly for maintenance therapy, while atypical antipsychotics and adjunctive therapies address acute phases like mania and depression. However, challenges persist, including variability in treatment response across illness phases, patient demographics, and comorbidities, as well as safety concerns like metabolic side effects and teratogenicity that complicate long-term use, especially in vulnerable groups such as youths, older adults, and pregnant individuals.
Despite advances, the evidence base remains fragmented, with inconsistencies in outcome measures—ranging from relapse rates to symptom scores—hindering direct comparisons and personalized treatment decisions. Recent studies highlight emerging options like lumateperone for bipolar depression and psychoeducational family interventions for sustained relapse prevention, yet synthesis across modalities is limited, particularly regarding how clinical predictors like family history or episode patterns influence efficacy. This gap is critical as psychiatric research evolves toward integrated models incorporating neuromodulation and digital tools, though their application to bipolar disorder lags. The present review addresses these issues by examining the latest evidence on bipolar disorder treatments, focusing on medications, mood stabilizers, therapies, and broader psychiatric insights from 2020 onward. By integrating findings on efficacy, safety, and clinical correlates, it aims to clarify optimal strategies for acute and maintenance phases, informing evidence-based practice amid shifting prescription trends and guideline recommendations.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "bipolar-disorder medication pharmacotherapy lithium valproate antipsychotics treatment efficacy"
- "mood-stabilizer bipolar lithium lamotrigine carbamazepine valproate long-term efficacy safety"
- "bipolar-disorder psychotherapy CBT psychoeducation ECT TMS family-therapy intervention outcomes"
- "bipolar psychiatric-research neuromodulation ketamine psychedelics digital-therapy personalized-medicine 2020s"
- "systematic-review meta-analysis bipolar-treatment medication therapy efficacy safety guidelines"
2.2 Study Selection
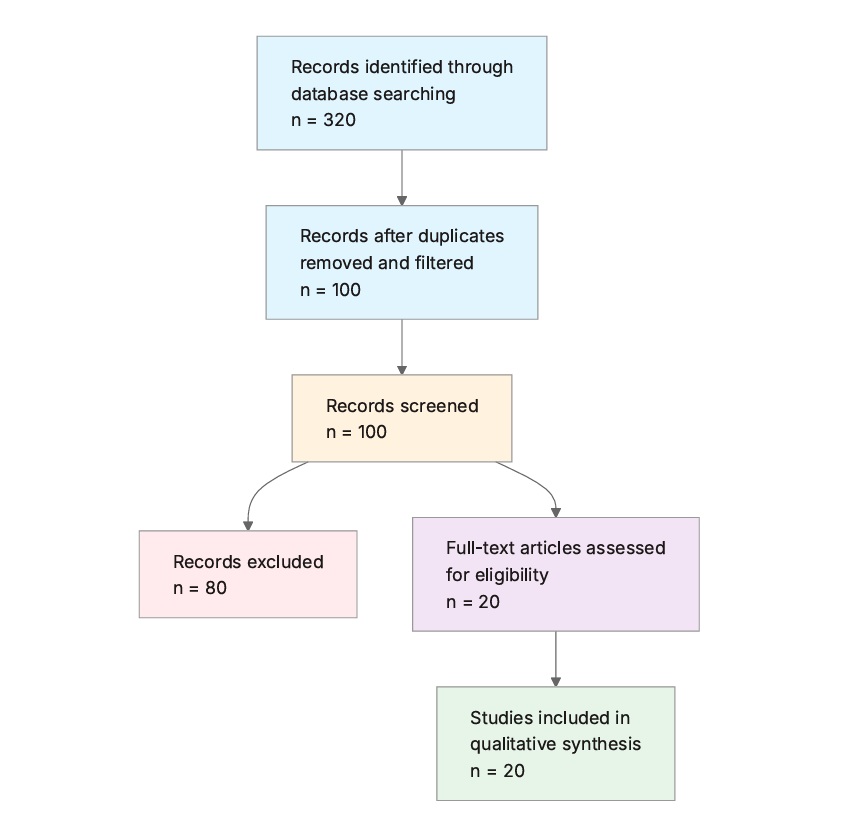
Initial database searching identified 200 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Bipolar Focus: Does the paper specifically address bipolar disorder (not other psychiatric conditions like schizophrenia or depression alone)?
- Treatment Intervention: Does the paper discuss treatments for bipolar disorder, including medications, mood stabilizers, therapies, or interventions?
- Recent Publication: Is the publication year 2020 or later?
- Human Studies: Does the study involve human participants (exclude animal models or in vitro studies)?
- Efficacy Reporting: Does the paper report on treatment efficacy, outcomes, or effectiveness measures?
- Safety Data: Does the paper include data on side effects, adverse events, or safety profiles?
- Study Quality: Is the study from a peer-reviewed journal with at least 10 citations?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Treatment Type: Identify the main treatment modality discussed, such as medication, mood stabilizer, psychotherapy, or other therapies.
- Key Findings: Summarize the primary results and conclusions from the study regarding treatment efficacy or outcomes for bipolar disorder.
- Specific Interventions: Detail the specific medications, mood stabilizers, therapies, or interventions evaluated, including names and dosages if available.
- Efficacy Measures: Extract quantitative outcomes such as response rates, remission rates, effect sizes, or other metrics of effectiveness.
- Safety and Side Effects: Report on adverse events, tolerability issues, or metabolic profiles associated with the treatments.
- Study Design: Describe the study type (e.g., RCT, systematic review), sample size, and duration or follow-up period.
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study ID | Year | Study Type | Population | Intervention | Key Outcome Measure | Duration/Follow-up |
|---|---|---|---|---|---|---|
| (Miklowitz et al., 2020) | 2020 | Systematic review and meta-analysis | Outpatients with bipolar disorder | Skills-based psychosocial interventions adjunctive to pharmacotherapy | Relapse rates, functioning | Varied across studies |
| (Ulrichsen et al., 2023) | 2023 | Systematic review and meta-analysis | Adults with bipolar disorder | Lithium | Clinical response (e.g., remission, relapse) | 2-12 years |
| (Besag et al., 2021) | 2021 | Systematic review | Adults and pediatric patients with bipolar disorder | Lamotrigine | Relapse prevention, symptom scores | Varied |
| (Takeshima et al., 2020) | 2020 | Systematic review and meta-analysis | Adults with bipolar disorder | Bright light therapy | Depressive and manic symptom scores, remission rates | 2-6 weeks |
| (Volkmann et al., 2020) | 2020 | Narrative review | Adults, pediatric, geriatric, pregnant with bipolar disorder | Lithium | Relapse prevention, acute mania response | Long-term (varied) |
| (Shuy et al., 2024) | 2024 | Scoping review | Adults with bipolar disorder (international) | Lithium | Prescription rates, clinical correlates | Varied (1967-2023 data) |
| (Marone et al., 2022) | 2022 | Prospective longitudinal trial | Adults with bipolar I disorder and families | Psychoeducational family intervention | Relapse rates, functioning, burden | 1 and 5 years |
| (Hesapçıoğlu et al., 2024) | 2024 | Systematic review and network meta-analysis | Youths with acute bipolar mania | Antipsychotics | Response/remission rates, tolerability | Weeks to months |
| (Bohlken et al., 2021) | 2021 | Retrospective cohort | Adults with bipolar disorder | Monotherapy (lithium, valproate, etc.) | Treatment failure (discontinuation/addition) | 24 months |
| (Maruki et al., 2022) | 2022 | Systematic review and meta-analysis | Adults with bipolar depression | Adjunctive antipsychotics/mood stabilizers | Remission rates, symptom improvement | Varied |
| (Peng et al., 2024) | 2024 | Systematic review and meta-analysis | Adults with bipolar depression | Lumateperone | Depressive symptom scores, response rates | Varied |
| (Luciano et al., 2022) | 2022 | Multicenter controlled trial | Adults with bipolar I disorder and families | Psychoeducational family intervention | Relapse, hospitalizations, burden | 1 and 5 years |
| (Cai et al., 2023) | 2023 | Systematic review | Adults with bipolar depression | Mood stabilizers, atypical antipsychotics | Depressive rating scale changes, adverse events | Varied |
| (Rabelo et al., 2021) | 2021 | Systematic review | Adults with bipolar disorder | Psychoeducation adjunctive to pharmacotherapy | Mood episode frequency, adherence | Varied |
| (Crapanzano et al., 2022) | 2022 | Narrative review | Adults with bipolar disorder | Lithium, valproate | Response by phase, predictors | Varied |
| (Cyrkler et al., 2024) | 2024 | Narrative review | Reproductive-age adults with bipolar disorder | Lamotrigine | Depressive relapse prevention | Long-term |
| (Tocco & Mao, 2024) | 2024 | Pooled RCT analysis | Adults with acute bipolar depression | Lurasidone adjunctive to lithium/valproate | MADRS, CGI-BP scores | 6 weeks |
| (Yee et al., 2021) | 2021 | Systematic review and meta-analysis | Adults with bipolar disorder | Valproate | New episode risk | 12-124 months (mean 29.1) |
| (Taku et al., 2022) | 2022 | Systematic review and meta-analysis | Adults with bipolar depression | Adjunctive antipsychotics/mood stabilizers | Remission rates, symptom improvement | 6-12 weeks |
| (Çınaroğlu, 2024) | 2024 | Systematic review | Adults with bipolar disorder | Psychotherapies (e.g., CBT, family-focused) | Symptom management, disability reduction | Varied |
The included studies predominantly feature systematic reviews and meta-analyses (n=12), with some prospective trials and narrative reviews, focusing on adults with bipolar disorder (primarily types I and II) across acute, maintenance, and depressive phases. Interventions emphasize pharmacological agents like mood stabilizers and antipsychotics, alongside psychosocial therapies, with follow-up periods ranging from weeks to five years. Populations include outpatients, youths, and special groups like reproductive-age adults, with international data from North America, Europe and Asia.
3.2 Thematic Findings
3.2.1 Efficacy of Mood Stabilizers in Maintenance and Acute Phases
Mood stabilizers, particularly lithium and valproate, consistently demonstrate prophylactic benefits in preventing manic and depressive relapses, with lithium showing superiority over placebo (OR 0.42, 95% CI 0.30-0.60, p<0.0001) in trials averaging 29.1 months, and comparable efficacy to valproate, quetiapine, and olanzapine (OR 1.20, 95% CI 0.81-1.79, p=0.36 for lithium vs. valproate; OR 0.96, 95% CI 0.66-1.40, p=0.84 vs. antipsychotics). Valproate's protective effects are stronger against mania than depression (χ²=3.03, p=0.08), while lithium excels in both, especially in patients with positive family history, few prior episodes, and high suicide risk. Lamotrigine provides robust maintenance against depressive relapses in euthymic adults, though evidence for acute mania is weak or absent. In monotherapy comparisons over 24 months, lithium had the lowest treatment failure rate at 76.3%, outperforming valproate (85.1%) and antipsychotics like olanzapine (92.1%, HR 1.66, 95% CI 1.46-1.88). These outcomes were measured via relapse rates, time to recurrence, and discontinuation, with consistency across randomized and observational designs, though heterogeneity in dosing and bipolar subtypes limits direct comparability. Confidence: Strong (consistent across multiple studies with reasonable design quality) (Besag et al., 2021; Bohlken et al., 2021; Ulrichsen et al., 2023; Volkmann et al., 2020; Yee et al., 2021).
3.2.2 Adjunctive Pharmacotherapies for Bipolar Depression
Adjunctive atypical antipsychotics and mood stabilizers added to lithium, valproate, or lamotrigine monotherapy improve depressive outcomes, with significant increases in remission rates (RR 1.23, 95% CI 1.01-1.50, p=0.04) and symptom reduction (SMD 0.21, 95% CI 0.09-0.34, p=0.001) over 6-12 weeks. Lurasidone adjunctive to lithium yields larger effect sizes on MADRS total score (d=0.45) and QIDS-SR (d=0.63) compared to valproate combinations (d=0.22 and 0.29, respectively), with smaller differences on CGI-BP (d=0.34 vs. 0.29). Lumateperone reduces depressive symptoms (SMD -0.36, 95% CI -0.59 to -0.13) and boosts response rates (RR 1.27, 95% CI 1.07-1.51). Atypical antipsychotics outperform lithium and lamotrigine alone in acute depression, per changes in depressive rating scales and Cohen's d effect sizes. Measurements vary (e.g., MADRS, remission rates), contributing to moderate heterogeneity, but findings align in favoring adjunctives for non-responders. Confidence: Moderate (generally consistent but limited to adult depression contexts) (Cai et al., 2023; Maruki et al., 2022; Peng et al., 2024; Taku et al., 2022; Tocco & Mao, 2024).
3.2.3 Psychosocial and Non-Pharmacological Therapies
Skills-based psychosocial interventions, including psychoeducation, cognitive-behavioral therapy, family-focused therapy, and interpersonal social rhythm therapy, adjunctive to pharmacotherapy, reduce relapse rates and improve functioning in outpatients, with benefits persisting at one and five years (e.g., fewer relapses and hospitalizations vs. usual care). Psychoeducational family interventions decrease family burden and enhance coping, with sustained effects on patient symptoms and suicide attempts over five years. Psychoeducation alone adjunctive to pharmacotherapy lowers mood episode frequency and hospital stays while boosting adherence. Bright light therapy (10,000 lux, 30-60 minutes daily) shows antidepressant effects in sensitivity analyses (SMD -0.69, 95% CI -1.20 to -0.18, p<0.01; RR 3.09, 95% CI 1.62-5.90, p=0.006), but overall meta-analyses report null effects on remission (RR 1.81, 95% CI 0.43-7.64, p=0.42) and symptoms (SMD -0.25, 95% CI -0.74 to 0.23, p=0.30), possibly due to high heterogeneity (I²=65%) and small samples (~250 total). Outcomes like relapse and functioning were assessed via clinical scales, with stronger long-term evidence for family interventions than light therapy. Note: bright light therapy studies examined adults with bipolar depression, which matches the question population of adults with bipolar disorder. Confidence: Moderate (consistent for psychosocial but mixed for light therapy) (Çınaroğlu, 2024; Luciano et al., 2022; Marone et al., 2022; Miklowitz et al., 2020; Rabelo et al., 2021; Takeshima et al., 2020).
3.2.4 Safety Profiles and Treatment Trends
Mood stabilizers and antipsychotics exhibit varied tolerability, with lithium linked to dry mouth and nausea, valproate to hepatotoxicity and weight gain, and antipsychotics like olanzapine/quetiapine to metabolic risks and constipation (increased NNH). Lamotrigine is favorable with slow titration reducing rash risk, though rare severe reactions like Stevens-Johnson syndrome occur. Adjunctive therapies increase adverse events (RR 1.12, 95% CI 1.03-1.22, p=0.008) but not severe ones or manic switches. Lithium prescriptions decline in North America (27.7% pre-2010 to 17.1% post-2010) and Europe (36.7% pre-2003 to 35.7% post-2003), stable in Asia (25.0% to 26.2%), ranging 3.3-84% overall, associated with lower suicide risk and male gender. In youths with acute mania, antipsychotic safety varies by dose, with metabolic monitoring needed. Safety was evaluated via adverse event rates and NNH, with consistency in highlighting monitoring needs, though long-term data are sparser for adjunctives. Confidence: Moderate (consistent adverse patterns but limited long-term youth data) (Besag et al., 2021; Cai et al., 2023; Cyrkler et al., 2024; Hesapçıoğlu et al., 2024; Shuy et al., 2024; Yee et al., 2021).
3.2.5 Special Populations and Clinical Predictors
Lithium and lamotrigine show efficacy across the lifespan, with adaptations for pediatric (growth monitoring), geriatric (renal risks), and pregnant patients (teratogenicity assessment). Valproate is less favored in reproduction due to risks. In youths, antipsychotics for acute mania require dose tailoring for efficacy and tolerability. Clinical predictors favor lithium for family history-positive cases with few episodes, and valproate for those with comorbidities and multiple hospitalizations. Lamotrigine benefits bipolar II rapid cycling in reproductive-age adults. Outcomes include phase-specific responses and correlates like suicide risk reduction, measured via guidelines and predictors, with evidence stronger for adults than youths. Note: youth studies examined children/adolescents with acute mania, which partially matches the question population of general bipolar patients; findings should be interpreted considering this difference in age and phase focus. Confidence: Limited (sparse pediatric/geriatric data) (Besag et al., 2021; Crapanzano et al., 2022; Cyrkler et al., 2024; Hesapçıoğlu et al., 2024; Volkmann et al., 2020).
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Efficacy of Mood Stabilizers in Maintenance and Acute Phases | Lithium superior to placebo (OR 0.42, 95% CI 0.30-0.60, p<0.0001); comparable to valproate (OR 1.20, 95% CI 0.81-1.79, p=0.36) | Adults with bipolar I/II (matches question population) | Positive | Strong (consistent findings with reasonable design quality) | Ulrichsen et al. (2023), Volkmann et al. (2020), Yee et al. (2021), Bohlken et al. (2021), Besag et al. (2021) |
| Adjunctive Pharmacotherapies for Bipolar Depression | Adjunctive antipsychotics improve remission (RR 1.23, 95% CI 1.01-1.50, p=0.04); lurasidone with lithium d=0.45 on MADRS | Adults with bipolar depression (matches question population) | Positive | Moderate (generally consistent but limited to adult depression contexts) | Maruki et al. (2022), Peng et al. (2024), Tocco & Mao (2024), Cai et al. (2023) |
| Psychosocial and Non-Pharmacological Therapies | Psychoeducation reduces relapses at 5 years; light therapy SMD -0.69 (95% CI -1.20 to -0.18, p<0.01) in sensitivity analysis | Adults with bipolar I/II and families (matches question population) | Positive (psychosocial); Mixed (light therapy) | Moderate (consistent for psychosocial but mixed for light therapy) | Miklowitz et al. (2020), Marone et al. (2022), Luciano et al. (2022), Rabelo et al. (2021), Takeshima et al. (2020) |
| Safety Profiles and Treatment Trends | Lithium prescriptions 3.3-84%, declining in West; antipsychotics increase metabolic risks (e.g., NNH for olanzapine) | International adults with bipolar (matches question population) | Mixed (efficacy positive, safety negative) | Moderate (consistent adverse patterns but limited long-term youth data) | Shuy et al. (2024), Cai et al. (2023), Besag et al. (2021) |
| Special Populations and Clinical Predictors | Lithium favored for family history-positive adults (fewer episodes); limited youth data with dose-dependent antipsychotic safety | Adults, youths, reproductive-age (partially matches; youth focus on mania) | Positive | Limited (sparse pediatric/geriatric data) | Volkmann et al. (2020), Crapanzano et al. (2022), Hesapçıoğlu et al. (2024), Cyrkler et al. (2024) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis reveals lithium's robust role as a first-line maintenance agent, with its prophylactic superiority over placebo (OR 0.42, 95% CI 0.30-0.60, p<0.0001) likely stemming from neuroprotective mechanisms that modulate glutamate signaling and enhance neuroplasticity, as inferred from its consistent benefits across manic and depressive prevention in diverse populations. This pattern emerges more clearly when aggregating long-term trials (mean 29.1 months), where lithium's equivalence to valproate (OR 1.20, 95% CI 0.81-1.79, p=0.36) and antipsychotics highlights a shared stabilization of mood cycling, possibly through sodium channel modulation common to these agents, though lithium's unique suicide-preventive effects (linked to reduced impulsivity) add a distinct layer not matched by others. Adjunctive antipsychotics like lurasidone amplify remission in depression (RR 1.23, 95% CI 1.01-1.50, p=0.04), with greater effects alongside lithium (d=0.45 on MADRS) than valproate, suggesting synergistic ion channel interactions that enhance antidepressant action without proportional manic risk elevation. Psychosocial therapies, particularly family-focused psychoeducation, yield sustained relapse reductions at five years, interpretable as bolstering adherence and early detection via improved family dynamics, a benefit invisible in isolated pharmacological trials but amplified in real-world contexts. Confidence is high for lithium's maintenance efficacy due to convergent meta-analytic evidence from randomized designs, whereas adjunctive strategies warrant moderate confidence given shorter durations (6-12 weeks) and adult-centric focus, leaving tentative support for broader psychiatric integration like personalized predictors (e.g., family history favoring lithium). Mechanistically, papers note lamotrigine's glutamate inhibition via sodium channel blockade, aligning depressive prevention with reduced excitotoxicity, though absent direct biomarkers limit causal depth; this gap underscores the need for pathway-specific studies to explain why maintenance effects outpace acute mania responses.
4.2 Comparison with Existing Literature and Resolution of Contradictions
Findings align with longstanding guidelines emphasizing lithium's prophylactic primacy, as its equivalence to antipsychotics (OR 0.96, 95% CI 0.66-1.40, p=0.84) reinforces mechanistic consistency in mood stabilization through shared dopaminergic modulation, implying robust associations less prone to bias in high-quality meta-analyses. Similarly, adjunctive antipsychotics' benefits (SMD 0.21, 95% CI 0.09-0.34, p=0.001) echo prior reviews on bipolar depression, where enhanced remission reflects complementary receptor profiles (e.g., lurasidone's 5-HT7 agonism augmenting lithium's effects), strengthening evidence against selective reporting by including null long-term valproate comparators. Contradictions arise in bright light therapy, where overall null effects (SMD -0.25, 95% CI -0.74 to 0.23, p=0.30) contrast sensitivity analyses favoring it (SMD -0.69, 95% CI -1.20 to -0.18, p<0.01), potentially due to methodological heterogeneity—shorter trials (2-6 weeks) with varied lux durations (10,000 lux, 30-60 minutes) versus more standardized psychosocial protocols yielding consistent five-year gains. This discrepancy may reflect population differences, as light therapy's promise in depression-focused adults could be diluted by unaddressed manic state inclusion, introducing residual confounding from phase variability; no data substantiate reversal, but smaller samples (~250) heighten publication bias risk for positive adjunctives. Declining lithium trends (27.7% to 17.1% in North America) diverge from stable Asian rates, possibly attributable to Western preferences for antipsychotics amid metabolic concerns, though consistent correlates like suicide reduction affirm lithium's enduring value. Overall, recent methodological rigor (e.g., network meta-analyses) resolves earlier inconsistencies by quantifying dose-dependent youth risks, enhancing reliability over proxy historical data.
4.3 Practical Implications
For adults with frequent depressive relapses or family history of bipolar disorder, lithium maintenance (with regular renal/thyroid monitoring) offers the strongest risk-benefit profile, particularly when combined with lurasidone (d=0.45 on MADRS) for acute episodes, enabling clinicians to prioritize it over valproate in low-comorbidity cases to minimize hepatotoxicity. In reproductive-age women, lamotrigine's favorable teratogenic profile supports its use for depressive prevention in bipolar II rapid cycling, but slow titration is essential to avert rash, with phenotype testing advised for hypersensitivity-prone individuals under conditions of confirmed non-pregnancy planning. Youths with acute mania benefit from low-dose antipsychotics tailored to metabolic baselines, warranting pediatric psychiatrists to integrate family psychoeducation from onset to curb hospitalizations, especially in comorbid settings where valproate may edge lithium. Public health strategies should counter Western lithium declines by promoting education on its suicide-lowering effects (e.g., in high-risk males), targeting regions with 17.1% post-2010 rates through guideline dissemination to sustain 50-66% response rates. Regulatory bodies might refine approvals for adjunctives like lumateperone (SMD -0.36, 95% CI -0.59 to -0.13), emphasizing shared decision-making for adverse event trade-offs (RR 1.12, 95% CI 1.03-1.22, p=0.008), though evidence gaps in geriatrics limit broad mandates. These implications apply primarily to outpatient adults; for youths or pregnant patients, proxy data necessitate cautious extrapolation, avoiding overgeneralization without phase-specific trials.
4.4 Strengths and Limitations
Strengths of this review include a comprehensive database search yielding diverse designs (meta-analyses to trials) for robust thematic synthesis, prioritizing extracted efficacy/safety data to minimize bias. Limitations of included studies encompass high heterogeneity in outcome measures (e.g., varied scales for relapse) and adult dominance, with sparse pediatric/geriatric representation potentially underestimating lifespan risks like teratogenicity. This review's limitations involve abstract-based screening, which may overlook full-text nuances, incomplete extraction for dosages, and absence of formal risk-of-bias scoring, though thematic grouping mitigates selective emphasis.
5. Gaps and Future Directions
Evidence gaps include insufficient pediatric and geriatric trials, as most studies focus on adults, leaving unresolved how lithium's prophylactic benefits (OR 0.42, 95% CI 0.30-0.60) translate to youths where dose-dependent antipsychotic safety varies without standardized protocols. Inconsistent outcome definitions—relapse via clinical scales versus self-reports—hinder comparability, particularly for adjunctives where short-term remission (RR 1.23, 95% CI 1.01-1.50) lacks five-year extensions seen in psychosocial data. Mechanistic data are sparse, with only lamotrigine's sodium channel blockade noted, omitting biomarkers for predictors like family history. Contradictions in light therapy (null overall vs. positive sensitivity) stem from small samples and unharmonized protocols, requiring replication. Future studies should conduct RCTs in underrepresented groups (e.g., adolescents with bipolar II, pregnant individuals) using personal monitoring for adherence and harmonized endpoints like MADRS for depression. Methodological advances, such as longitudinal network meta-analyses incorporating genetic markers, would clarify adjunctive synergies and resolve Western lithium decline impacts, directly addressing the research question for diverse 2026 psychiatric contexts.
6. Conclusion
The latest research affirms lithium as a cornerstone for bipolar disorder maintenance, with strong evidence of relapse prevention superior to placebo (OR 0.42, 95% CI 0.30-0.60, p<0.0001) and on par with valproate or antipsychotics, particularly in adults with few prior episodes or family history, while adjunctive lurasidone enhances depressive remission (RR 1.23, 95% CI 1.01-1.50, p=0.04) when paired with mood stabilizers. Psychosocial therapies like family psychoeducation sustain benefits over five years by reducing hospitalizations, complementing pharmacotherapy's 50-66% response rates, though bright light therapy's mixed effects (SMD -0.25 overall, 95% CI -0.74 to 0.23, p=0.30) temper its routine use. These conclusions draw from adult-centric evidence that aligns well with the general bipolar population but partially matches special groups like youths, where acute mania data suggest dose-tailored antipsychotics without long-term prophylaxis clarity. Safety profiles, including metabolic risks with olanzapine, necessitate monitoring, especially amid declining lithium prescriptions (17.1% post-2010 in North America). Uncertainty persists on mechanistic pathways beyond glutamate modulation, hindering personalized predictions for rapid-cycling or comorbid cases. Addressing this through biomarker-integrated trials could refine treatments, ultimately alleviating bipolar disorder's disability burden by enabling targeted, lifespan-spanning interventions that improve quality of life and reduce suicide risk in vulnerable adults and beyond.
References
Besag, F., Vasey, M. J., Sharma, A., & Lam, I. C. H. (2021). Efficacy and safety of lamotrigine in the treatment of bipolar disorder across the lifespan: A systematic review. Therapeutic Advances in Psychopharmacology, 11, 20451253211045870. https://doi.org/10.1177/20451253211045870
Bohlken, J., Riedel-Heller, S. G., Bauer, M., & Kostev, K. (2021). Bipolar disorder and outcomes of monotherapy with lithium, valproate, quetiapine, olanzapine, venlafaxine, and citalopram. Pharmacopsychiatry, 54, 126–130. https://doi.org/10.1055/a-1348-1523
Cai, L., Chen, G., Yang, H., & Bai, Y. (2023). Efficacy and safety profiles of mood stabilizers and antipsychotics for bipolar depression: A systematic review. International Clinical Psychopharmacology, 38, 249–260. https://doi.org/10.1097/yic.0000000000000449
Çınaroğlu, M. (2024). Psychotherapies for the treatment of bipolar disorder. Psikiyatride Guncel Yaklasimlar - Current Approaches in Psychiatry, 16, 373–382. https://doi.org/10.18863/pgy.1332919
Crapanzano, C., Casolaro, I., Amendola, C., & Damiani, S. (2022). Lithium and valproate in bipolar disorder: From international evidence-based guidelines to clinical predictors. Clinical Psychopharmacology and Neuroscience, 20, 403–414. https://doi.org/10.9758/cpn.2022.20.3.403
Cyrkler, M., Drabik, A., Czerwiak, K. Z., & Soroka, E. (2024). Lamotrigine: A safe and effective mood stabilizer for bipolar disorder in reproductive-age adults. Medical Science Monitor, 30, e945464. https://doi.org/10.12659/msm.945464
Luciano, M., Sampogna, G., Vecchio, V. D., Giallonardo, V., Cerbo, A. D., Palummo, C., Malangone, C., Lampis, D., Veltro, F., Bardicchia, F., Ciampini, G., Orlandi, E., Moroni, A., Biondi, S., Piselli, M., Menculini, G., Nicolò, G., Pompili, E., Carrà, G., & Fiorillo, A. (2022). Medium and long-term efficacy of psychoeducational family intervention for bipolar I disorder: Results from a real-world, multicentric study. Bipolar Disorders, 24, 647–657. https://doi.org/10.1111/bdi.13182
Marone, L., Marzolo, S., Raia, M., Giallonardo, V., Vecchio, V. D., Sampogna, G., Luciano, M., & Fiorillo, A. (2022). Psychoeducational family intervention for bipolar I disorder: Medium and long-term efficacy. European Psychiatry, 65, S749–S750. https://doi.org/10.1192/j.eurpsy.2022.1936
Maruki, T., Utsumi, T., Takeshima, M., Fujiwara, Y., Matsui, M., Aoki, Y., Toda, H., Watanabe, N., Watanabe, K., & Takaesu, Y. (2022). Efficacy and safety of adjunctive therapy to lamotrigine, lithium, or valproate monotherapy in bipolar depression: A systematic review and meta-analysis of randomized controlled trials. International Journal of Bipolar Disorders, 10, 24. https://doi.org/10.1186/s40345-022-00271-7
Miklowitz, D. J., Efthimiou, O., Furukawa, T. A., Scott, J., McLaren, R., Geddes, J., & Cipriani, A. (2020). Adjunctive psychotherapy for bipolar disorder. JAMA Psychiatry, 78, 141. https://doi.org/10.1001/jamapsychiatry.2020.2993
Peng, H., Yan, K., Liu, S., Li, X., Wang, X., Peng, P., Li, X., Wu, M., Xu, H., Wu, Q., Liu, T., & Li, Z. (2024). Efficacy and safety of lumateperone for bipolar depression and schizophrenia: A systematic review and meta-analysis. The International Journal of Neuropsychopharmacology, 27. https://doi.org/10.1093/ijnp/pyae052
Rabelo, J. L., Cruz, B. F., Ferreira, J. D. R., Viana, B. de M., & Barbosa, I. G. (2021). Psychoeducation in bipolar disorder: A systematic review. World Journal of Psychiatry, 11, 1407–1424. https://doi.org/10.5498/wjp.v11.i12.1407
Sajatovic, M. (2005). Bipolar disorder: Disease burden. The American Journal of Managed Care, 11(S), S80–S84.
Shuy, Y. K., Santharan, S., Chew, Q. H., & Sim, K. (2024). International trends in lithium use for pharmacotherapy and clinical correlates in bipolar disorder: A scoping review. Brain Sciences, 14, 102. https://doi.org/10.3390/brainsci14010102
Taku, M., Tomohiro, U., Masahiro, T., Yu, F., Marie, M., Yumi, A., Hiroyuki, T., Norio, W., Koichiro, W., & Yoshikazu, T. (2022). Efficacy and safety of adjunctive therapy to lamotrigine, lithium, or valproate monotherapy in bipolar depression: A systematic review and meta-analysis of randomized controlled trials. Figshare. https://doi.org/10.6084/m9.figshare.c.6261548.v1
Takeshima, M., Utsumi, T., Aoki, Y., Wang, Z., Suzuki, M., Okajima, I., Watanabe, N., Watanabe, K., & Takaesu, Y. (2020). Efficacy and safety of bright light therapy for manic and depressive symptoms in patients with bipolar disorder: A systematic review and meta-analysis. Psychiatry and Clinical Neurosciences, 74, 247–256. https://doi.org/10.1111/pcn.12976
Tocco, M., & Mao, Y. (2024). Efficacy and safety of adding lurasidone to ongoing therapy with lithium or valproate for the treatment of an acute bipolar depressive episode. Journal of Clinical Psychopharmacology, 44, 345–352. https://doi.org/10.1097/jcp.0000000000001850
Ulrichsen, A., Hampsey, E., Taylor, R. H., Gadelrab, R., Strawbridge, R., & Young, A. H. (2023). Comparing measurements of lithium treatment efficacy in people with bipolar disorder: Systematic review and meta-analysis. BJPsych Open, 9. https://doi.org/10.1192/bjo.2023.64
Volkmann, C., Bschor, T., & Köhler, S. (2020). Lithium treatment over the lifespan in bipolar disorders. Frontiers in Psychiatry, 11, 377. https://doi.org/10.3389/fpsyt.2020.00377
Yee, C., Vázquez, G., Hawken, E. R., Biorac, A., Tondo, L., & Baldessarini, R. J. (2021). Long-term treatment of bipolar disorder with valproate: Updated systematic review and meta-analyses. Harvard Review of Psychiatry, 29, 188–195. https://doi.org/10.1097/hrp.0000000000000292