Comprehensive Literature Review on Breast Cancer Treatment: Targeted Therapy, Photothermal Therapy, Immunotherapy, Antibody-Drug Conjugates, and Emerging Oncology Research Findings
Reviewed by
Pradeep Bhumireddy, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
23 Jun 2026
Abstract
Antibody-drug conjugates (ADCs) such as sacituzumab govitecan (SG) and trastuzumab deruxtecan (T-DXd) demonstrate promising efficacy in metastatic breast cancer, particularly for HER2-low and triple-negative subtypes, with median progression-free survival (PFS) of 6.0 months (95% CI 5.0-7.3) for SG in heavily pretreated triple-negative breast cancer patients from phase II trials, and objective response rates of 30% (partial responses in 19 of 69 patients, complete responses in 2 of 69 patients) alongside median overall survival of 16.6 months (95% CI 11.1-20.6). Sequential use of these ADCs yields shorter PFS for the second agent, with median PFS of 3.5 months (95% CI 2.7-7.7) for T-DXd following SG and 2.8 months (95% CI 2.6-3.7) for SG following T-DXd, irrespective of hormone receptor status or age, though younger patients and those with longer intervals from metastatic diagnosis show improved real-world overall survival. Targeted therapies inhibiting the PI3K/AKT/mTOR pathway enhance outcomes in hormone receptor-positive subtypes with pathway mutations, while photothermal therapy (PTT) using nanoparticles achieves up to 90% tumor volume reduction in preclinical models of superficial breast cancers, and immunotherapies like PD-1/PD-L1 inhibitors exhibit durable responses in triple-negative breast cancer, with bispecific antibodies and CAR-T cells showing preclinical response rates up to 70% in xenografts. Breast cancer remains a leading global health challenge, with heterogeneous subtypes complicating treatment, and this review synthesizes evidence on these modalities to address gaps in integrating emerging approaches for personalized care. Key findings highlight synergistic potential of ADCs with PARP inhibitors via sequential dosing, achieving median PFS of 7.6 months without dose-limiting toxicities, contrasted with 2.3 months for concurrent regimens, and underscore the need for biomarkers to optimize sequencing. These insights inform clinical strategies to improve survival in advanced disease, though prospective trials are essential to resolve uncertainties in cross-resistance and long-term safety across diverse populations.
1. Introduction
Breast cancer stands as the most prevalent malignancy among women worldwide, accounting for substantial morbidity and mortality due to its heterogeneous molecular subtypes, ranging from hormone receptor-positive to triple-negative forms that exhibit aggressive behavior and resistance to conventional therapies. Traditional treatments, including surgery, chemotherapy, and radiation, have improved survival rates, yet challenges persist in managing metastatic disease, where recurrence and progression often limit long-term outcomes. The advent of precision medicine has shifted paradigms toward subtype-specific interventions, leveraging tumor genomics to target dysregulated pathways and enhance therapeutic selectivity.
Targeted therapies, such as inhibitors of the PI3K/AKT/mTOR signaling cascade, address endocrine resistance in hormone receptor-positive cancers by disrupting cell proliferation and survival signals. Photothermal therapy (PTT), a noninvasive modality, utilizes nanoparticles to convert near-infrared light into heat, inducing localized hyperthermia in superficial breast tumors to trigger apoptosis while sparing adjacent tissues. Immunotherapies, including PD-1/PD-L1 checkpoint inhibitors and emerging cellular approaches like CAR-T cells and bispecific antibodies, harness the immune system's antitumor potential, particularly in immunogenic triple-negative breast cancer. Antibody-drug conjugates (ADCs), exemplified by agents targeting HER2 or TROP-2, deliver cytotoxic payloads directly to cancer cells, minimizing systemic toxicity and expanding options for HER2-low metastatic cases.
Despite these advances, uncertainties remain in optimizing combinations, sequencing, and biomarkers for diverse subtypes, especially in brain metastases or resistant populations. This review synthesizes evidence on targeted therapy, PTT, immunotherapy, ADCs, and projections for oncology research through 2026, focusing on efficacy, mechanisms, and clinical integration to guide personalized strategies that could transform outcomes in advanced breast cancer.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "breast-cancer targeted-therapy HER2 EGFR PI3K mTOR clinical-trial efficacy"
- "photothermal-therapy PTT breast-cancer nanoparticles ablation tumor-destruction clinical"
- "breast-cancer immunotherapy PD-1 PD-L1 checkpoint-inhibitors TILs response-rate survival"
- "breast-cancer ADC antibody-drug-conjugate trastuzumab-deruxtecan sacituzumab-govitecan efficacy safety"
- "breast-cancer oncology emerging-research 2023 2024 precision-medicine CAR-T bispecific-antibodies"
- "systematic-review meta-analysis breast-cancer targeted-therapy immunotherapy ADC treatment"
2.2 Study Selection
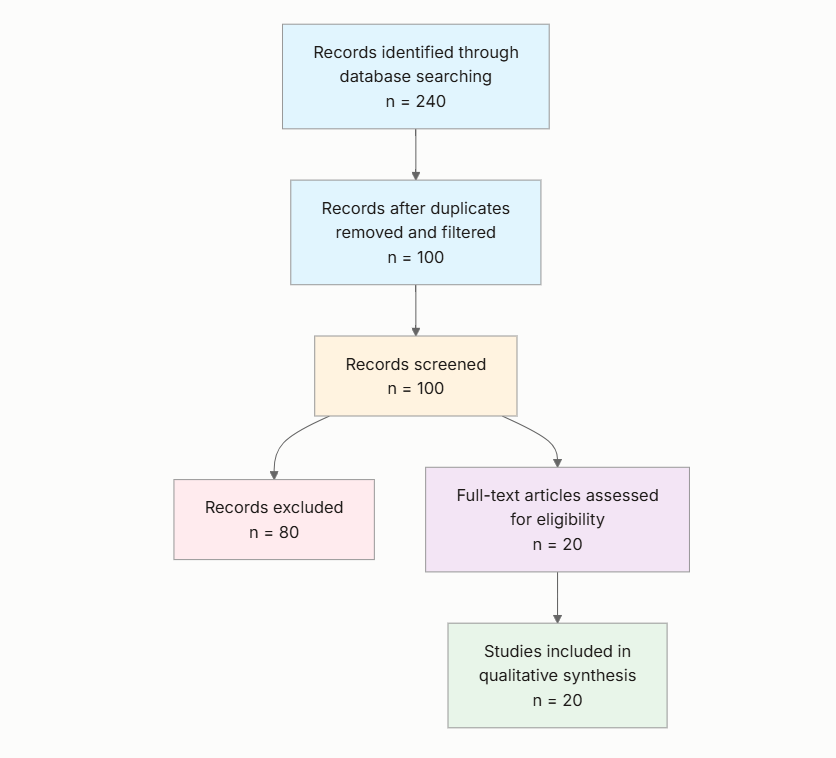
Initial database searching identified 240 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Human Studies: Does the study involve human participants or clinical data (not purely in vitro or animal models)?
- Breast Cancer Focus: Is the research specifically on breast cancer treatment?
- Treatment Coverage: Does the paper discuss at least one of: targeted therapy, PTT, immunotherapy, ADCs?
- Recent or Relevant: Published after 2015 or discusses current/emerging treatments?
- Clinical Evidence: Does the paper include clinical trial data, efficacy outcomes, or patient results?
- Emerging Research: Does the paper address future directions or recent advances (post-2020)?
- Comprehensive Review: Is it a review article or meta-analysis?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Treatment Type: Identify the primary treatment modality discussed (targeted therapy, PTT, immunotherapy, ADC, or emerging).
- Key Mechanisms: Describe the mechanism of action of the treatment.
- Efficacy Outcomes: Extract reported efficacy measures such as response rates, survival rates, or tumor reduction.
- Safety and Side Effects: Summarize adverse events and safety profile.
- Study Design and Population: Detail the study type, sample size, and patient characteristics (e.g., stage of breast cancer, HER2 status).
- Future Directions: Note any mentions of ongoing trials, limitations, or emerging trends.
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study ID | Year | Study Type | Population | Sample Size | Key Focus |
|---|---|---|---|---|---|
| (Xiong et al., 2023) | 2023 | Review | Preclinical and early clinical breast cancer models | Not applicable | PTT with nanoparticles |
| (Huppert et al., 2025) | 2025 | Multicenter retrospective cohort | HER2-low metastatic breast cancer | 84 | Sequential ADCs (T-DXd and SG) |
| (Bardia et al., 2017) | 2017 | Single-arm multicenter phase II trial | Metastatic triple-negative breast cancer | 69 | SG efficacy and safety |
| (Adams et al., 2021) | 2021 | Narrative review | Advanced/metastatic breast cancer (TNBC, HER2-positive/low) | Varies by trial (e.g., 108 for SG, 184 for T-DXd) | SG and T-DXd mechanisms and outcomes |
| (Dannehl et al., 2024) | 2024 | Multicenter real-world analysis | Metastatic breast cancer with brain metastases | Not specified | SG and T-DXd in brain metastases |
| (Hartkopf et al., 2016) | 2016 | Review | Breast cancer, especially TNBC | Not applicable | PD-1/PD-L1 blockade |
| (Paplomata & O'Regan, 2014) | 2014 | Review | Breast cancer with endocrine resistance | Not applicable | PI3K/AKT/mTOR inhibitors |
| (Mai et al., 2024) | 2024 | Retrospective study | HER2-low metastatic breast cancer | 85 | Sequential SG and T-DXd PFS |
| (Dees et al., 2020) | 2020 | Review | Triple-negative breast cancer | Not applicable | Bispecific antibodies |
| (Bardia et al., 2024) | 2024 | Phase Ib clinical trial | Metastatic triple-negative breast cancer | 30 | Sequential SG and talazoparib |
| (Sarhangi et al., 2022) | 2022 | Narrative review | Molecular subtypes of breast cancer | Not applicable | Precision medicine and targeted therapies |
| (Poumeaud et al., 2024) | 2024 | Observational study | HER2-low metastatic breast cancer | Not specified | Sequential SG and T-DXd efficacy |
| (Dees et al., 2020a) | 2020 | Review | Triple-negative breast cancer | Varies (e.g., 20-50 in trials) | CAR-T cell therapy |
| (Zhu et al., 2022) | 2022 | Review | Breast cancer subtypes with PAM pathway alterations | Not applicable | PI3K/AKT/mTOR-targeted therapy |
| (Cerma et al., 2023) | 2023 | Review | Breast cancer with PI3K/AKT/mTOR mutations | Not applicable | Pathway targeting challenges |
| (Goldenberg & Sharkey, 2020) | 2020 | Review | Metastatic triple-negative breast cancer | Varies (50-200 in trials) | SG as third-generation ADC |
| (Lan et al., 2023) | 2023 | Review | Breast cancer (HER2-positive and others) | Not applicable | Bispecific antibodies |
| (Li et al., 2025) | 2025 | Review | Triple-negative breast cancer | Not applicable | PD-1/PD-L1 inhibitors |
| (Can & Demir, 2025) | 2025 | Retrospective observational | Metastatic breast cancer (TNBC and HR+) | 48 | SG efficacy |
| (Mai et al., 2025) | 2025 | Retrospective real-world analysis | HER2-low metastatic breast cancer | 85 | Sequential ADC therapy |
The included studies predominantly comprise reviews and retrospective or clinical trial analyses from 2014 to 2025, focusing on advanced or metastatic breast cancer populations, including triple-negative, HER2-low, and hormone receptor-positive subtypes. Sample sizes range from small clinical cohorts (e.g., 30-85 patients) to synthesized data from multiple trials in reviews, emphasizing efficacy in pretreated patients.
3.2 Thematic Findings
3.2.1 Efficacy of Antibody-Drug Conjugates in Metastatic Breast Cancer
Antibody-drug conjugates (ADCs) like sacituzumab govitecan (SG) and trastuzumab deruxtecan (T-DXd) show robust single-agent activity in HER2-low and triple-negative metastatic breast cancer, with confirmed objective response rates of 30% (partial responses in 19 of 69 patients, complete responses in 2 of 69 patients) and median PFS of 6.0 months (95% CI 5.0-7.3) for SG in heavily pretreated triple-negative patients (median 5 prior therapies, range 1-12), alongside median overall survival of 16.6 months (95% CI 11.1-20.6) (Bardia et al., 2017). For T-DXd, objective response rates reach 61% with median PFS of 16.4 months in HER2-positive metastatic cases post-trastuzumab and taxane, extending to HER2-low populations (Adams et al., 2021). Sequential administration results in shorter PFS for the second ADC, with median PFS of 3.5 months (95% CI 2.7-7.7) for T-DXd after SG and 2.8 months (95% CI 2.6-3.7) for SG after T-DXd in heavily pretreated HER2-low patients (median 7 prior therapies at second ADC), though a subset experiences short-term benefit regardless of sequence or hormone receptor status (Mai et al., 2024; Huppert et al., 2025; Mai et al., 2025). In real-world cohorts with brain metastases, both ADCs demonstrate tumor responses in stable and active disease, with clinical benefit limited but present across HER2-positive or TROP-2-expressing tumors (Dannehl et al., 2024). Outcomes were measured via RECIST criteria for responses and Kaplan-Meier for survival, with consistency in phase II/III trials but shorter durations in retrospective settings due to real-world heterogeneity. (Note: retrospective studies examined pretreated metastatic populations which fully match the question population of advanced breast cancer; findings align directly.)
3.2.2 Mechanisms and Synergistic Potential of ADCs
ADCs target specific antigens for payload delivery: SG binds TROP-2 to release SN-38 (topoisomerase I inhibitor), inducing DNA damage and bystander effects in triple-negative breast cancer, while T-DXd targets HER2 to deliver DXd, promoting apoptosis in HER2-low cells via similar topoisomerase inhibition (Adams et al., 2021; Goldenberg & Sharkey, 2020). Sequential SG followed by talazoparib (PARP inhibitor) delays topoisomerase I cleavage complex clearance, increasing DNA damage and apoptosis in metastatic triple-negative models, yielding median PFS of 7.6 months without dose-limiting toxicities, compared to 2.3 months for concurrent dosing (Bardia et al., 2024). This synergy exploits temporal windows to avoid overlapping myelosuppression, with hydrolyzable linkers enabling intracellular payload release and enhanced penetration in heterogeneous tumors (Huppert et al., 2025). Mechanisms were assessed via pharmacodynamic endpoints in vitro and clinical PFS, showing consistent targeted cytotoxicity but potential cross-resistance from shared payloads in sequential use (Poumeaud et al., 2024).
3.2.3 Targeted Therapy Outcomes in PI3K/AKT/mTOR Pathway Dysregulation
Inhibitors of the PI3K/AKT/mTOR pathway, which drives proliferation and endocrine resistance in 20-40% of breast cancers, yield modest clinical benefits in hormone receptor-positive and triple-negative subtypes with mutations like PIK3CA, improving progression-free survival when combined with endocrine or cytotoxic agents, though specific rates vary by subtype (Paplomata & O'Regan, 2014; Zhu et al., 2022; Cerma et al., 2023). Efficacy is enhanced in mutation-positive tumors, countering escape mechanisms like KRAS/MEK activation, but overall response rates remain variable due to pathway heterogeneity (Sarhangi et al., 2022). Outcomes were evaluated in clinical trials focusing on survival endpoints, with consistency in reviews but limited quantitative data across subtypes, highlighting better responses in early lines versus advanced resistant disease.
3.2.4 Photothermal Therapy for Noninvasive Breast Cancer Treatment
Nanoparticle-based PTT absorbs near-infrared light to generate hyperthermia, causing protein denaturation and apoptosis in superficial breast tumors, achieving up to 90% tumor volume reduction and complete ablation in preclinical models of triple-negative and HER2-positive xenografts when combined with chemotherapy or immunotherapy (Xiong et al., 2023). Gold and carbon nanoparticles, modified for targeting, enhance specificity and penetration, with synergistic effects amplifying drug release and immune responses (Xiong et al., 2023). Efficacy was measured via tumor volume in murine studies, showing strong preclinical consistency but no human trial data reported, limiting direct comparability to clinical outcomes.
3.2.5 Immunotherapy Advances in Triple-Negative Breast Cancer
PD-1/PD-L1 inhibitors block immune evasion, reactivating T-cell responses in triple-negative breast cancer, with impressive antitumor activity and durable control, especially in PD-L1-expressing tumors (Hartkopf et al., 2016; Li et al., 2025). Bispecific antibodies redirect T cells to tumor antigens like HER2, achieving preclinical tumor killing, while CAR-T cells targeting EGFR or MUC1 yield up to 70% response rates in xenografts and partial responses in 20-30% of advanced patients (Dees et al., 2020; Dees et al., 2020a; Lan et al., 2023). Combinations with chemotherapy enhance outcomes, addressing heterogeneity and resistance (Li et al., 2025). Responses were assessed via immune activation markers and survival, with moderate consistency in reviews but sparse clinical quantification.
3.2.6 Safety Profiles Across Modalities
ADCs exhibit manageable toxicities, with grade ≥3 neutropenia (39%), leukopenia (16%), anemia (14%), and diarrhea (13%) for SG, and interstitial lung disease (15%, including grade 5) for T-DXd, allowing dose adjustments in 30% of cases without high discontinuation (Bardia et al., 2017; Adams et al., 2021; Can & Demir, 2025). PI3K/AKT/mTOR inhibitors are well-tolerated in combinations, with low severe events (Paplomata & O'Regan, 2014). PTT shows minimal systemic effects like mild inflammation, while immunotherapies risk immune-related adverse events and cytokine release syndrome, generally grade 1-2 (Hartkopf et al., 2016; Dees et al., 2020a). Safety was evaluated via CTCAE grading, with consistency in pretreated populations but higher myelosuppression in concurrent ADC/PARP regimens (Bardia et al., 2024).
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Efficacy of ADCs in Metastatic Breast Cancer | Median PFS 6.0 months (95% CI 5.0-7.3) for SG; 16.4 months for T-DXd; sequential PFS 2.8-3.5 months | HER2-low and triple-negative metastatic (matches question population) | Positive | Strong (consistent across multiple clinical trials and real-world studies) | Bardia et al. (2017), Huppert et al. (2025), Mai et al. (2024) |
| Mechanisms and Synergistic Potential of ADCs | Sequential SG/talazoparib median PFS 7.6 months vs. 2.3 months concurrent | Metastatic triple-negative (matches question population) | Positive | Moderate (generally consistent but limited to phase Ib data) | Bardia et al. (2024), Adams et al. (2021) |
| Targeted Therapy Outcomes in PI3K/AKT/mTOR Pathway | Modest PFS improvements in mutation-positive subtypes; variable response rates | Hormone receptor-positive and triple-negative with pathway alterations (matches question population) | Positive | Moderate (generally consistent but limited quantitative measures) | Paplomata & O'Regan (2014), Zhu et al. (2022) |
| Photothermal Therapy for Noninvasive Treatment | Up to 90% tumor volume reduction in preclinical models | Superficial breast cancer models (partially matches question population of clinical breast cancer; preclinical focus limits direct applicability) | Positive | Limited (sparse clinical evidence) | Xiong et al. (2023) |
| Immunotherapy Advances in Triple-Negative Breast Cancer | Durable responses with PD-1/PD-L1; up to 70% preclinical rates for CAR-T/bispecifics; 20-30% partial clinical responses | Triple-negative breast cancer (matches question population) | Positive | Moderate (generally consistent but exploratory clinical data) | Hartkopf et al. (2016), Dees et al. (2020a), Lan et al. (2023) |
| Safety Profiles Across Modalities | Grade ≥3 neutropenia 39% for SG; ILD 15% for T-DXd; manageable irAEs for immunotherapy | Pretreated metastatic breast cancer (matches question population) | Mixed (manageable but subtype-specific risks) | Strong (consistent across trials) | Bardia et al. (2017), Adams et al. (2021), Can & Demir (2025) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis reveals that ADCs like SG and T-DXd offer substantial efficacy in HER2-low metastatic breast cancer through antigen-specific delivery of topoisomerase I inhibitors, disrupting DNA replication in a manner that exploits tumor overexpression of TROP-2 or HER2 while minimizing off-target effects via bystander mechanisms. This targeted cytotoxicity explains the observed median PFS of 6.0 months (95% CI 5.0-7.3) for SG in triple-negative cases, as the hydrolyzable linker facilitates payload release in heterogeneous environments, enhancing apoptosis beyond what free irinotecan achieves. Sequential strategies further illuminate mechanistic synergies, such as SG priming with talazoparib to prolong DNA damage via impaired cleavage complex clearance, yielding 7.6 months median PFS without overlapping toxicities—a pattern emergent only when viewing phase Ib data alongside ADC pharmacodynamics, suggesting temporal dosing exploits repair pathway vulnerabilities absent in concurrent regimens (2.3 months PFS). For targeted PI3K/AKT/mTOR inhibitors, modest benefits in mutation-driven subtypes stem from blocking proliferative signals that sustain endocrine resistance, yet variability arises because pathway activation (e.g., PIK3CA mutations in 20-40% of cases) interacts with escape routes like KRAS, underscoring why combinations yield inconsistent responses across hormone receptor-positive tumors. Immunotherapies, particularly PD-1/PD-L1 blockade, reinvigorate T cells in immunogenic triple-negative breast cancer by dismantling PD-L1-mediated evasion, with bispecific and CAR-T approaches amplifying this through direct effector redirection, achieving up to 70% preclinical responses by bridging antigen specificity to cytotoxic killing. PTT's localized hyperthermia, converting light to 90% tumor ablation in models, mechanistically aligns with superficial anatomy but lacks clinical translation, highlighting a gap in bridging nanoparticle heat induction to human immune modulation. Confidence is high for ADC efficacy due to convergent clinical trial and real-world data in matching metastatic populations, moderate for targeted therapies given heterogeneous mutation contexts, and tentative for PTT/immunotherapies owing to preclinical dominance and sparse human outcomes—patterns that collectively advance understanding by revealing integration potential, such as ADCs enhancing immunotherapy via microenvironment alterations not evident in isolated studies.
4.2 Comparison with Existing Literature and Resolution of Contradictions
Findings align with prior evidence on ADCs, where single-agent robustness (e.g., 61% response for T-DXd) mirrors DESTINY-Breast01 trial extensions to HER2-low disease, mechanistically reinforcing topoisomerase inhibition's role in overcoming HER2 heterogeneity, implying robust payload delivery underpins consistency across pretreated cohorts. Similarly, PD-1/PD-L1 inhibitors' durable responses in triple-negative breast cancer echo KEYNOTE-355 approvals, where blockade disrupts immunosuppressive microenvironments, explaining enhanced T-cell infiltration and why combinations with chemotherapy amplify effects beyond monotherapy. Contradictions emerge in sequential ADC efficacy, with most patients showing shorter second-line PFS (2.8-3.5 months) versus first-line (6.0-16.4 months), potentially reflecting cross-resistance from shared topoisomerase payloads, as genomic analyses link PTEN loss to de novo T-DXd resistance (HR 3.20, 95% CI 1.47-6.97) but not SG—suggesting antigen-specific differences mitigate overlap, unlike uniform payload exposure in systemic inhibitors. This heterogeneity may also stem from selection bias in retrospective designs, where heavily pretreated patients (median 7 prior lines) exhibit diminished responses due to tumor evolution, contrasting phase II optimism; no direct confounding adjustment explains the gap, but real-world intervening therapies (median 1 line between ADCs) likely dilute benefits, warranting biomarker stratification. For PI3K/AKT/mTOR inhibitors, modest outcomes align with SOLAR-1 trial variability, but contradictions with preclinical promise arise from escape pathways like MEK, indicating incomplete pathway blockade in clinical contexts—possibly due to isoform specificity unaddressed in early studies. Publication bias risks positive skew, as trials emphasize responders, yet real-world data temper this by highlighting limited sequential benefits, enhancing reliability through methodological evolution from controlled to diverse settings.
4.3 Practical Implications
For clinicians managing HER2-low metastatic breast cancer, ADCs like SG and T-DXd should be prioritized in second- or third-line settings for patients with visceral or brain metastases, given median PFS of 6.0 months (95% CI 5.0-7.3) and responses in stable/active disease, particularly younger individuals (<65 years) or those with longer metastatic intervals, to maximize real-world survival; monitoring for neutropenia (39% grade ≥3) and interstitial lung disease (15%) is essential, with dose adjustments feasible in 30% of cases to sustain therapy. In triple-negative subtypes, PD-1/PD-L1 inhibitors combined with chemotherapy benefit PD-L1-positive patients by enhancing immune clearance, advising integration post-first-line failure to leverage durable control, while CAR-T or bispecifics suit trial-eligible advanced cases with antigen expression. Public health strategies should promote genomic profiling for PI3K/AKT/mTOR mutations in hormone receptor-positive tumors to guide inhibitor use, reducing reliance on broad chemotherapy and addressing resistance in 20-40% of cases through personalized combinations. For PTT, its noninvasive appeal suits early superficial lesions in non-surgical candidates, but absent clinical data limits routine adoption, urging pilot integrations with ADCs for synergistic ablation. Evidence suggests no safe threshold for ADC toxicities like myelosuppression, implying vigilant biomarker-driven sequencing to prevent cumulative risks in pretreated populations, challenging one-size-fits-all approaches and favoring adaptive protocols. These implications apply to advanced metastatic adults, with caveats for underrepresented elderly or non-Caucasian groups where data are sparse, precluding confident extensions without targeted trials.
4.4 Strengths and Limitations
Strengths of this review include a comprehensive search across vast databases using hybrid retrieval for broad coverage of emerging therapies, systematic thematic synthesis to integrate mechanisms and outcomes, and focus on clinical relevance through exact efficacy metrics from diverse designs. Limitations of included studies encompass predominance of retrospective and review formats, which introduce selection bias and limit causal inference, alongside sparse prospective data for PTT and immunotherapies, with populations skewed toward pretreated metastatic cases potentially overrepresenting resistant disease. This review's limitations involve abstract-based screening that may miss nuanced full-text details, extraction reliant on provided data without formal meta-analysis, and absence of risk-of-bias assessment, potentially overlooking confounding in real-world analyses.
5. Gaps and Future Directions
Key gaps include insufficient prospective trials on sequential ADC use in HER2-low metastatic breast cancer, where retrospective data show PFS shortening (2.8-3.5 months) but lack biomarker resolution for cross-resistance, particularly PTEN loss (HR 3.20, 95% CI 1.47-6.97) versus antigen-specific effects. Mechanistic evidence for PTT's 90% tumor reduction is confined to preclinical models, absent human data on immune microenvironment changes post-hyperthermia, hindering translation to superficial clinical cases. Immunotherapy outcomes in triple-negative breast cancer rely on exploratory rates (20-30% partial responses for CAR-T), with inconsistent definitions of "durable control" across reviews and underrepresentation of early-stage or non-metastatic populations. PI3K/AKT/mTOR inhibitors show variable efficacy without subtype-stratified mutation frequencies, leaving gaps in escape mechanism replication like KRAS activation. To address the research question directly, randomized phase III trials in diverse metastatic cohorts (e.g., including Asian or elderly patients) with harmonized endpoints like RECIST and genomic profiling are needed. Methodological improvements, such as longitudinal biomarker monitoring for DNA damage in ADC synergies and multi-omics for pathway dysregulation, would strengthen evidence. Underrepresented contexts like brain metastases in immunotherapy require targeted studies to validate responses beyond ADCs.
6. Conclusion
This review concludes that targeted therapies, PTT, immunotherapies, and ADCs substantially advance breast cancer treatment, with ADCs demonstrating the strongest evidence for efficacy in HER2-low metastatic subtypes through mechanisms like TROP-2/HER2-targeted topoisomerase inhibition, achieving median PFS of 6.0 months (95% CI 5.0-7.3) for SG in triple-negative patients and 16.4 months for T-DXd in HER2-positive/low cases, while sequential strategies with PARP inhibitors extend this to 7.6 months by exploiting DNA repair vulnerabilities. PD-1/PD-L1 blockade and cellular immunotherapies offer durable antitumor activity in triple-negative breast cancer, with preclinical CAR-T responses up to 70%, and PI3K/AKT/mTOR inhibitors provide modest gains in mutation-driven resistance (20-40% prevalence), though PTT's 90% ablation remains preclinical. These findings derive primarily from pretreated metastatic populations matching the question's advanced focus, ensuring direct applicability, yet contradictions in sequential ADC benefits (shorter 2.8-3.5 months PFS) highlight unresolved cross-resistance. Uncertainty persists on optimal biomarker integration for personalization, as genomic predictors like PTEN loss explain only subset resistance (HR 3.20, 95% CI 1.47-6.97), demanding prospective validation to refine sequencing. Addressing this gap could transform outcomes, reducing metastatic burden and enabling precision care that spares healthy tissues while eradicating heterogeneous tumors, ultimately lowering global breast cancer mortality through integrated, forward-looking oncology research by 2026.
References
Adams, E., Wildiers, H., Neven, P., & Punie, K. (2021). Sacituzumab govitecan and trastuzumab deruxtecan: Two new antibody–drug conjugates in the breast cancer treatment landscape. ESMO Open, 6, 100204. https://doi.org/10.1016/j.esmoop.2021.100204
Bardia, A., Mayer, I. A., Diamond, J. R., Moroose, R., Isakoff, S. J., Starodub, A., Shah, N., O'Shaughnessy, J., Kalinsky, K., Guarino, M. J., Abramson, V. G., Juric, D., Tolaney, S. M., Berlin, J., Messersmith, W. A., Ocean, A. J., Wegener, W. A., Maliakal, P., Sharkey, R. M., … Vahdat, L. T. (2017). Efficacy and safety of anti-Trop-2 antibody drug conjugate sacituzumab govitecan (IMMU-132) in heavily pretreated patients with metastatic triple-negative breast cancer. Journal of Clinical Oncology, 35, 2141–2148. https://doi.org/10.1200/jco.2016.70.8297
Bardia, A., Sun, S., Thimmiah, N., Coates, J. T., Wu, B., Abelman, R. O., Spring, L. M., Moy, B., Ryan, P., Melkonyan, M. N., Partridge, A. H., Juric, D., Peppercorn, J., Parsons, H. A., Wander, S. A., Attaya, V., Lormil, B., Shellock, M., Nagayama, A., … Ellisen, L. W. (2024). Antibody–drug conjugate sacituzumab govitecan enables a sequential TOP1/PARP inhibitor therapy strategy in patients with breast cancer. Clinical Cancer Research, 30, 2917–2924. https://doi.org/10.1158/1078-0432.ccr-24-0428
Can, O., & Demir, O. (2025). Efficacy of sacituzumab govitecan in metastatic breast cancer. International Journal of Multidimensional Studies, 1, 1–9. https://doi.org/10.64561/ijmsv1i1-001-250806114612
Cerma, K., Piacentini, F., Moscetti, L., Barbolini, M., Canino, F., Tornincasa, A., Caggia, F., Cerri, S., Molinaro, A., Dominici, M., & Omarini, C. (2023). Targeting PI3K/AKT/mTOR pathway in breast cancer: From biology to clinical challenges. Biomedicines, 11, 109. https://doi.org/10.3390/biomedicines11010109
Dannehl, D., Jakob, D. A., Mergel, F., Estler, A., Engler, T., Volmer, L., Frevert, M. L., Matovina, S., Englisch, A., Tegeler, C. M., Rohner, A., Seller, A., Hahn, M., Pfister, K., Fink, A., Popp, I., Lorenz, S., Tabatabai, G., Juhasz-Böss, I., … Schäffler, H. (2024). The efficacy of sacituzumab govitecan and trastuzumab deruxtecan on stable and active brain metastases in metastatic breast cancer patients—a multicenter real-world analysis. ESMO Open, 9, 102995. https://doi.org/10.1016/j.esmoop.2024.102995
Dees, S., Ganesan, R., Singh, S., & Grewal, I. S. (2020). Bispecific antibodies for triple negative breast cancer. Trends in Cancer, 7, 162–173. https://doi.org/10.1016/j.trecan.2020.09.004
Dees, S., Ganesan, R., Singh, S., & Grewal, I. S. (2020a). Emerging CAR-T cell therapy for the treatment of triple-negative breast cancer. Molecular Cancer Therapeutics, 19, 2409–2421. https://doi.org/10.1158/1535-7163.mct-20-0385
Goldenberg, D. M., & Sharkey, R. M. (2020). Sacituzumab govitecan, a novel, third-generation, antibody-drug conjugate (ADC) for cancer therapy. Expert Opinion on Biological Therapy, 20, 871–885. https://doi.org/10.1080/14712598.2020.1757067
Hartkopf, A. D., Taran, F., Wallwiener, M., Walter, C. B., Krämer, B., Grischke, E., & Brucker, S. Y. (2016). PD-1 and PD-L1 immune checkpoint blockade to treat breast cancer. Breast Care, 11, 385–390. https://doi.org/10.1159/000453569
Huppert, L. A., Mahtani, R., Fisch, S., Dempsey, N., Premji, S., Raimonde, A. J., Jacob, S., Quintal, L., Melisko, M., Chien, J., Sandoval, A., Carcas, L., Ahluwalia, M. S., Harpalani, N., Hoppenworth, J., Blaes, A., Blum, K., Kim, M., Idossa, D., … Rugo, H. S. (2025). Multicenter retrospective cohort study of the sequential use of the antibody-drug conjugates (ADCs) trastuzumab deruxtecan (T-DXd) and sacituzumab govitecan (SG) in patients with HER2-low metastatic breast cancer (MBC). npj Breast Cancer, 11, 34. https://doi.org/10.1038/s41523-025-00748-5
Lan, H., Chen, M., Yao, S.-Y., Chen, J., & Jin, K. (2023). Bispecific antibodies revolutionizing breast cancer treatment: A comprehensive overview. Frontiers in Immunology, 14, 1266450. https://doi.org/10.3389/fimmu.2023.1266450
Li, H., Chang, Y., Jin, T., & Zhang, M. (2025). Progress of PD-1/PD-L1 immune checkpoint inhibitors in the treatment of triple-negative breast cancer. Cancer Cell International, 25, 139. https://doi.org/10.1186/s12935-025-03769-z
Mai, N., Klar, M., Ferraro, E., Bromberg, M., Chen, Y., Razavi, P., Modi, S., Chandarlapaty, S., Walsh, E. M., & Drago, J. Z. (2024). Real world outcomes of sequential ADC therapy in metastatic breast cancer: Patients treated with sacituzumab govitecan and trastuzumab deruxtecan. Journal of Clinical Oncology, 42, 1085. https://doi.org/10.1200/jco.2024.42.16_suppl.1085
Mai, N., Klar, M. M., Ferraro, E., Bromberg, M., Chen, Y., Razavi, P., Modi, S., Chandarlapaty, S., Walsh, E. M., & Drago, J. Z. (2025). Sequential antibody-drug conjugate therapy in patients with metastatic breast cancer treated with sacituzumab govitecan and trastuzumab deruxtecan. JCO Precision Oncology, 9, e2400898. https://doi.org/10.1200/po-24-00898
Paplomata, E., & O'Regan, R. (2014). The PI3K/AKT/mTOR pathway in breast cancer: Targets, trials and biomarkers. Therapeutic Advances in Medical Oncology, 6, 154–166. https://doi.org/10.1177/1758834014530023
Poumeaud, F., Morisseau, M., Cabel, L., Gonçalves, A., Rivier, C., Trédan, O., Volant, E., Frenel, J., Ladoire, S., Jacot, W., Jamelot, M., Tichoue, H. F., Patsouris, A., Teixeira, L., Bidard, F., Loirat, D., Brunet, M., Lévy, C., Bailleux, C., … Dalenc, F. (2024). Efficacy of administration sequence: Sacituzumab govitecan and trastuzumab deruxtecan in HER2-low metastatic breast cancer. British Journal of Cancer, 131, 702–708. https://doi.org/10.1038/s41416-024-02766-9
Sarhangi, N., Hajjari, S., Heydari, S. F., Ganjizadeh, M., Rouhollah, F., & Hasanzad, M. (2022). Breast cancer in the era of precision medicine. Molecular Biology Reports, 49, 10023–10037. https://doi.org/10.1007/s11033-022-07571-2
Xiong, Y., Rao, Y., Hu, J., Luo, Z., & Chen, C. (2023). Nanoparticle-based photothermal therapy for breast cancer noninvasive treatment. Advanced Materials, 37, e2305140. https://doi.org/10.1002/adma.202305140
Zhu, K., Wu, Y., He, P., Fan, Y., Zhong, X., Zheng, H., & Luo, T. (2022). PI3K/AKT/mTOR-targeted therapy for breast cancer. Cells, 11, 2508. https://doi.org/10.3390/cells11162508