Latest Research on COVID Vaccines 2026: Efficacy and Safety Across Variants, Boosters, and Emerging Vaccine Platforms
Reviewed by
Pradeep Bhumireddy, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
23 Jun 2026
Abstract
Current evidence indicates that COVID-19 vaccines remain effective at preventing symptomatic and severe disease, while safety profiles are generally acceptable across platforms, though immune protection is clearly shaped by age, boosting, variant exposure, and vaccine type. In randomized and systematic evidence, mRNA vaccines (against pre-Omicron variants) show higher efficacy than adenovirus-vectored vaccines, with pooled estimates of 94.6% (95% CI 0.936–0.954) versus 80.2% (95% CI 0.56–0.93), and bivalent mRNA boosters provide superior protection against severe Omicron outcomes than original monovalent boosters across age groups (Pormohammad et al., 2021; Song et al., 2024). These findings matter because the clinical question has shifted from initial authorization to durability, immune escape, and how best to tailor boosters for vulnerable populations. Across laboratory and clinical studies, Delta breakthrough infection generally induces broader and stronger neutralizing responses than Omicron breakthrough infection, while more recent XBB.1.5 booster exposure yields robust neutralization against newer lineages including JN.1 (Servellita et al., 2022; Springer et al., 2024). Safety findings are reassuring overall: serious adverse events were probably low and broadly similar between vaccine and placebo groups, and newer comparative booster trials reported mainly mild-to-moderate reactogenicity with very few vaccine-related serious adverse events (Graña et al., 2022; Ho et al., 2024). However, the evidence base is still uneven for long-term protection, variant-adapted boosters, and detailed safety profiles in underrepresented populations such as children, adolescents, cancer patients, and other special groups, so 2026-relevant conclusions remain partly inferential rather than definitive.
1. Introduction
COVID-19 vaccination has remained one of the central interventions for reducing infection, symptomatic disease, hospitalization, and death, yet the evidence base has evolved from initial efficacy trials into a more complex landscape shaped by immune escape from variants, repeated boosting, and heterogeneous host responses. Early randomized trials established that several vaccine platforms could prevent clinical COVID-19, but these studies often had short follow-up, limited representation of pregnant individuals, immunocompromised patients, and previously infected people, and were conducted before later variants substantially altered the antigenic landscape (Graña et al., 2022; Sharif et al., 2021). As the pandemic progressed, the key questions shifted from whether vaccines work at all to how well they continue to work against Omicron lineages, how durable protection remains after primary series or booster doses, and whether updated or variant-adapted formulations offer meaningful advantages.
Safety remains an equally important dimension because vaccination campaigns have extended to adolescents, children, medically complex groups, and previously vaccinated adults receiving additional doses. Across the reviewed literature, vaccine safety is usually reported in terms of reactogenicity, serious adverse events, and selected rare events such as myocarditis or pericarditis, although the depth of reporting varies substantially by design and population (Lv et al., 2021; Fendler et al., 2022). Immunogenicity studies add another layer of understanding by showing that neutralizing antibody responses are not uniform across variants or exposure histories, with breakthrough infection and boosting often producing different breadth and magnitude of response (Servellita, Syed, Morris, et al., 2022; Zhu et al., 2023).
The present review therefore addresses the current state of evidence on COVID-19 vaccine efficacy and safety with emphasis on clinical effectiveness, long-term safety, variant-related immune escape, booster performance, and emerging vaccine platforms relevant to 2026. Rather than treating efficacy and safety as fixed properties of a vaccine, this synthesis considers them as context-dependent outcomes shaped by platform, schedule, host factors, and the evolving viral landscape.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "COVID-19 vaccine efficacy safety clinical-trial immunogenicity effectiveness 2026"
- "COVID-vaccine long-term safety adverse-events reactogenicity pharmacovigilance myocarditis"
- "COVID-vaccine variants booster effectiveness neutralization Omicron breakthrough infection"
- "COVID-vaccine 2026 mRNA protein-subunit variant-adapted next-generation platform"
- "systematic-review meta-analysis COVID-vaccine efficacy safety booster variant"
2.2 Study Selection
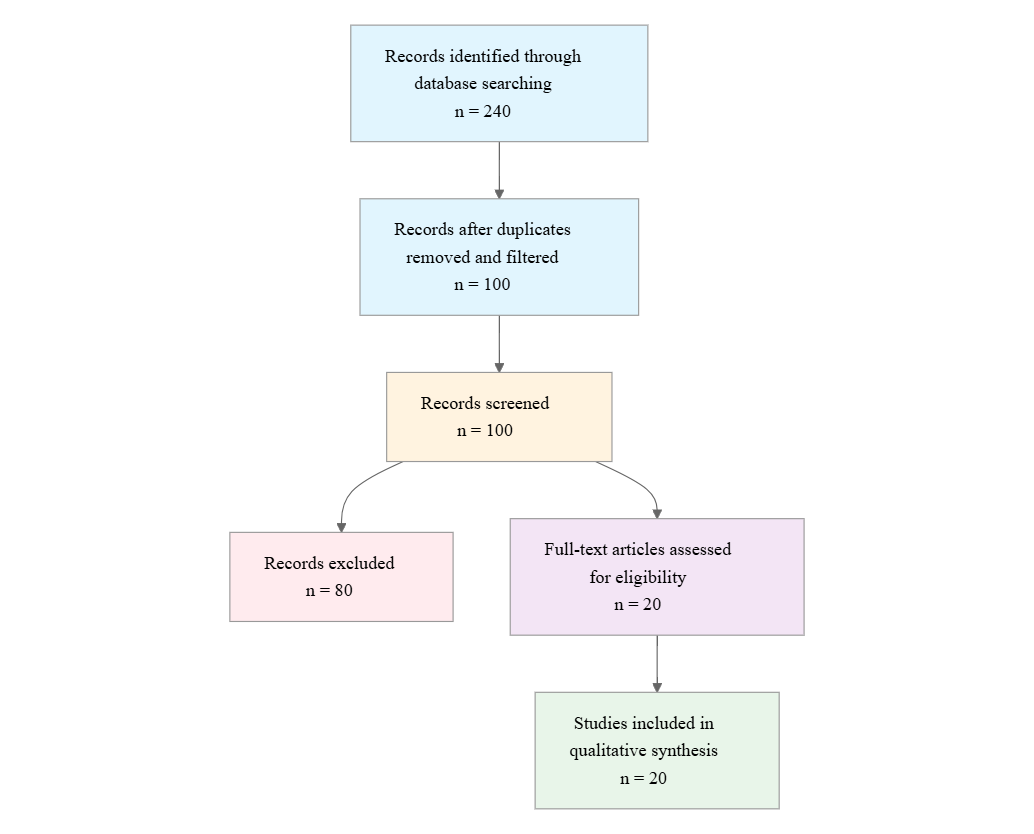
Initial database searching identified 200 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Human Study: Does the study involve human participants or human-derived surveillance data rather than only animal, in vitro, or computational modeling?
- COVID Vaccine: Does the study evaluate a COVID-19 vaccine, booster, vaccine update, or vaccine platform intended for SARS-CoV-2 prevention?
- Efficacy Outcome: Does the study report vaccine efficacy, vaccine effectiveness, immunogenicity, neutralization, breakthrough infection, hospitalization, severe disease, or death outcomes?
- Safety Outcome: Does the study report adverse events, reactogenicity, serious adverse events, myocarditis/pericarditis, or other safety findings?
- Variant/Booster Context: Does the study address variants, booster doses, updated formulations, waning immunity, or immune escape?
- Long-term Follow-up: Does the study include follow-up of at least 3 months or longer-term safety/durability assessment?
- 2026-Relevant: Does the study report recent vaccine research, updated formulations, or findings published in 2024-2026?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on vaccine platform, study design, population, efficacy/effectiveness, variant and booster context, safety findings, long-term follow-up, and key conclusions. Thematic analysis was used to synthesize patterns across studies, prioritizing quantitative findings where available and treating immunologic neutralization outcomes separately from clinical effectiveness endpoints.
3. Results
3.1 Characteristics of Included Studies
| Study and Year | Study Type | Population | Intervention/Comparator | Primary Focus | Key Outcome Type |
|---|---|---|---|---|---|
| Frenck et al. 2021 | Phase 3 randomized trial | Adolescents 12–15 years | BNT162b2 | Safety, immunogenicity, efficacy | Clinical efficacy and immune response |
| Pormohammad et al. 2021 | Systematic review/meta-analysis | Trial participants | mRNA and adenovirus-vectored vaccines | Efficacy, side effects, immunogenicity | Pooled efficacy and safety |
| Sharif et al. 2021 | Systematic review/meta-analysis | Phase I–III trial participants, adults emphasized | Multiple platforms | Efficacy, immunogenicity, safety | Pooled efficacy and reactogenicity |
| Xing et al. 2021 | Systematic review | General vaccine literature | Multiple vaccines | Efficacy and safety | Narrative synthesis |
| Lv et al. 2021 | Systematic review | Children and adolescents <18 years | Multiple vaccines | Safety, immunogenicity, efficacy | Pediatric/adolescent outcomes |
| Graña et al. 2022 | Cochrane systematic review | RCT participants | Multiple vaccines vs placebo | Efficacy and safety | Confirmed symptomatic and severe disease |
| Yan et al. 2021 | Narrative review | Multiple populations | Twelve vaccines | Safety and efficacy | Trial-based synthesis |
| Beladiya et al. 2023 | Systematic review/meta-analysis | Controlled and randomized trial participants | Multiple vaccine platforms | Incidence of COVID-19, safety | Comparative platform efficacy |
| Fendler et al. 2022 | Review | Patients with cancer | Multiple platforms, primary and booster vaccination | Immunogenicity, efficacy, safety | Oncology-focused synthesis |
| Chenchula et al. 2022 | Systematic review | Booster-eligible vaccinated populations | Booster doses | Omicron booster effectiveness | Booster effectiveness against Omicron |
| Krammer & Ellebedy 2023 | Conceptual review | Not specified | Variant-adapted booster concept | Updated boosters for future variants | Forward-looking synthesis |
| Servellita et al. 2022 | Laboratory cohort | Vaccinated individuals with Delta or Omicron breakthrough infection | Breakthrough infection status | Neutralization breadth and potency | Neutralizing titers |
| Lechmere et al. 2022 | Laboratory cohort | Vaccinated individuals with Delta breakthrough infection | Breakthrough infection status | Breadth against variants including Omicron | Neutralizing titers |
| Zhu et al. 2023 | Laboratory immunology study | Vaccinated and breakthrough-infected individuals | CoronaVac, ZF2001 booster, hybrid immunity | Durability against Omicron subvariants | Neutralization durability |
| Springer et al. 2024 | Laboratory immunology study | Individuals with diverse vaccination/infection histories | XBB.1.5 booster or infection | Neutralization of JN.1 and related variants | Neutralizing antibodies |
| Chew et al. 2024 | Phase 3 non-inferiority RCT | Adults previously vaccinated with three doses | Inhaled Ad5-nCoV-IH vs intramuscular BNT-IM | Safety, efficacy, immunogenicity | Antibody and safety outcomes |
| Ho et al. 2024 | Phase 3 randomized trial | Adults 18–85 years | ARCT-154 vs ChAdOx1-S | Safety, immunogenicity, efficacy | Clinical and immune outcomes |
| Song et al. 2024 | Systematic review/meta-analysis | Booster recipients across age groups | Bivalent mRNA vs monovalent boosters | Severe Omicron outcomes | Comparative effectiveness |
| 2021 review on COVID-19 vaccines | Systematic review | General populations | Broad vaccine review | Efficacy and safety | Narrative synthesis |
| 2022 cancer review | Review | Patients with cancer | Vaccination and boosters | Immunogenicity, efficacy, safety | Specialty population synthesis |
Overall, the evidence spans randomized efficacy trials, systematic reviews, meta-analyses, clinical reviews, and laboratory immunology studies. The clinical trial evidence is strongest for primary vaccination and booster effectiveness, whereas the variant-focused literature is dominated by neutralization studies rather than clinical endpoints. Several studies address proxy populations rather than the general adult population, including adolescents, children, patients with cancer, and previously vaccinated adults receiving booster formulations, which is important when interpreting applicability.
3.2 Thematic Findings
3.2.1 Primary vaccine efficacy is consistently favorable, with mRNA platforms generally outperforming adenovirus-vectored vaccines
Across clinical trials, COVID-19 vaccines reduce symptomatic infection and, for some products, severe or critical disease, with the clearest pooled advantage observed for mRNA platforms. One meta-analysis reported efficacy of 94.6% (95% CI 0.936–0.954) for mRNA-based vaccines and 80.2% (95% CI 0.56–0.93) for adenovirus-vectored vaccines (Pormohammad et al., 2021). A separate synthesis similarly reported 85% (95% CI 82–88) efficacy for mRNA vaccines and 73% (95% CI 69–77) for adenovirus-vector vaccines in adults ≥18 years (Sharif et al., 2021). In trial-based pediatric and adolescent evidence, BNT162b2 showed high efficacy in adolescents 12–15 years, and NVX-CoV2373 in adolescents (12–17 years) achieved 79.5% efficacy (95% CI 46.8%–92.1%) against mild COVID-19, with Delta-specific efficacy of 82.0% (95% CI 32.4%–95.2%) (Frenck et al., 2021; Áñez et al., 2023). (Note: these studies examined adolescents and adult trial participants, which partially match the question population of the general COVID vaccine population; findings should be interpreted considering this difference.)
Confidence: Strong for the direction of benefit, moderate for direct cross-platform ranking because outcome definitions and eras differ. The consistency of benefit across randomized and pooled evidence supports robust clinical effectiveness, but exact comparability is limited by different variants, schedules, and endpoints.
3.2.2 Booster vaccination improves protection against Omicron, especially when the booster is variant-adapted
The booster literature indicates that immunity after a two-dose series wanes against Omicron, but third doses restore protection, particularly against severe outcomes. A systematic review focused on Omicron booster effectiveness reported that protection against hospitalization and death decreases slowly after a two-dose schedule and that booster vaccination is important in the Omicron setting (Chenchula et al., 2022). More directly, bivalent mRNA boosters have demonstrated higher effectiveness against severe Omicron-associated outcomes than prior monovalent mRNA booster doses in pooled analyses across age groups, with particularly important benefits observed for older adults (Song et al., 2024). Clinical trial evidence also suggests that booster-type strategies can preserve efficacy while altering immunogenicity: in a phase 3 trial, an inhaled Ad5-nCoV-IH booster induced lower immunogenicity than intramuscular tozinameran, yet the reported efficacy against variants was comparable, and adverse drug reactions were less frequent with the inhaled vaccine (39.26%) than with BNT-IM (64.68%) (Chew et al., 2024). (Note: these studies examined booster-eligible populations and, in one case, adults previously vaccinated with three COVID-19 doses; findings should be interpreted considering this difference relative to the broader general population.)
Confidence: Moderate to strong for the conclusion that boosting improves protection, and moderate for superiority of bivalent formulations because the comparative evidence is stronger than the product-specific evidence but remains constrained by observational synthesis and evolving variant exposure.
3.2.3 Variant exposure reshapes neutralizing immunity, with Delta generally eliciting broader responses than Omicron, and XBB.1.5 booster exposure restoring breadth against newer lineages
Laboratory immunology studies consistently show that the quality of neutralization depends on the infecting or boosting variant. Delta breakthrough infection in vaccinated individuals produced markedly stronger neutralizing activity than Omicron breakthrough infection: one study reported WT titers rising 57-fold after Delta breakthrough versus only a 5.8-fold increase after Omicron breakthrough infection (Servellita et al., 2022). In a related cohort, uninfected, non-boosted individuals had VLP neutralization titers reduced 2.7-fold against Delta and 15.4-fold against Omicron versus wild-type, whereas boosted individuals had 18-fold increased titers, and Omicron breakthrough infection yielded only 0.32-fold titers relative to boosted controls (Servellita, Syed, Morris, et al., 2022). A broader comparison found Delta breakthrough infection induced 10.8-fold higher WT titers than Omicron in immunocompetent, unboosted patients (p = 0.037), with smaller Omicron-associated responses potentially linked to a higher proportion of mild or asymptomatic infections (55.0% versus 28.6%) (Servellita et al., 2022). More recent work extends this pattern into the XBB and JN.1 era: a monovalent XBB.1.5 booster or XBB.1.5 breakthrough infection generated robust antibody levels against all variants tested, whereas JN.1 evaded antibodies after single BA.1, BA.2, or BA.5 breakthrough infections (Springer et al., 2024). (Note: these studies examined vaccinated individuals with breakthrough infection or booster exposure, which partially matches the question population of vaccine recipients; findings should be interpreted considering this difference because they assess immunologic correlates rather than direct clinical effectiveness.)
Confidence: Strong for the direction of variant-dependent neutralization; limited for translating neutralization to clinical protection because outcomes are laboratory-based and not directly linked to disease endpoints.
3.2.4 Durability is variable: vaccination alone wanes against Omicron subvariants, whereas hybrid immunity is more persistent
Durability data indicate that antibody responses after vaccination alone decline substantially against later Omicron lineages, but hybrid immunity is more resilient. In one study, a two-dose CoronaVac series or a third-dose ZF2001 booster elicited limited neutralization against Omicron subvariants at 6 months, including BA.1, BA.2, BA.2.75, BA.4/BA.5, BF.7, BQ.1.1, and XBB (Zhu et al., 2023). The same study reported that hybrid immunity and breakthrough infections with Delta, BA.1, or BA.2 induced long-term persistence of antibody responses, with over 70% of sera neutralizing BA.1, BA.2, BA.4/BA.5, and BF.7, although BQ.1.1 and XBB were more resistant, showing neutralizing titer reductions of approximately 9- to 41-fold, 16- to 63-fold, and 4- to 25-fold, respectively (Zhu et al., 2023). This theme is echoed by booster-focused reviews noting that protection from severe outcomes diminishes after two doses and that updated boosters remain necessary in the Omicron era (Chenchula et al., 2022; Song et al., 2024). (Note: this study examined vaccinated and breakthrough-infected individuals with specific CoronaVac/ZF2001 and hybrid-immunity histories, which partially matches the question population of all COVID vaccine recipients; findings should be interpreted considering this difference.)
Confidence: Moderate. The durability signal is coherent, but much of the detailed evidence is immunologic rather than clinical and is concentrated in specific vaccine histories.
3.2.5 Safety findings are broadly reassuring, though reporting depth varies substantially by platform and population
Across trial syntheses, serious adverse events were usually uncommon and similar to placebo, and newer randomized comparisons found that both safety and reactogenicity were acceptable. The Cochrane review reported probably little or no difference between most vaccines and placebo for serious adverse events (Graña et al., 2022). In a phase 3 trial comparing ARCT-154 with ChAdOx1-S, both vaccines were well tolerated, with mainly mild-to-moderate solicited adverse events and few related serious adverse events (Ho et al., 2024). In adolescents, NVX-CoV2373 reactogenicity was largely mild to moderate and transient, serious adverse events were rare and balanced between groups, and no adverse events led to discontinuation (Áñez et al., 2023). Pediatric systematic review evidence also noted injection-site pain, fatigue, headache, and chest pain as common adverse events, with a limited number of myocarditis and pericarditis cases reported (Lv et al., 2021). However, many reviews and trials do not provide detailed adverse-event rates in the supplied data, limiting direct comparison across platforms. (Note: these studies examined adults, adolescents, and children rather than a single homogeneous population; findings should be interpreted considering this difference.)
Confidence: Moderate to strong for overall safety reassurance, but limited for rare-event precision because the included evidence is unevenly reported and often not powered for uncommon adverse events.
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Primary efficacy is favorable, especially for mRNA vaccines | mRNA efficacy 94.6% (95% CI 0.936–0.954) vs adenovirus-vectored 80.2% (95% CI 0.56–0.93) | Mostly adults and trial participants; partially matches general vaccine population | Positive | Strong | Pormohammad et al. (2021), Sharif et al. (2021), Frenck et al. (2021) |
| Boosters improve Omicron-era protection | Bivalent mRNA boosters showed superior protection against severe outcomes than original monovalent boosters | Booster recipients, especially older adults; partially matches general vaccine population | Positive | Moderate | Song et al. (2024), Chenchula et al. (2022), Chew et al. (2024) |
| Variant exposure changes neutralization breadth | Delta breakthrough produced 57-fold WT titer increases; Omicron breakthrough only 5.8-fold | Vaccinated individuals with breakthrough infection; proxy population for immune response | Positive but variant-dependent | Strong | Servellita et al. (2022), Servellita, Syed, Morris, et al. (2022), Lechmere et al. (2022) |
| Durability is weaker after vaccination alone | CoronaVac or ZF2001 showed limited neutralization at 6 months against Omicron subvariants | Vaccinated and hybrid-immunity cohorts; proxy population for durability | Negative for waning, positive for hybrid immunity | Moderate | Zhu et al. (2023), Chenchula et al. (2022) |
| Safety is broadly acceptable | Serious adverse events probably little or no different from placebo; mild-to-moderate reactogenicity common | Adults, adolescents, and children; partially matches general vaccine population | Neutral to positive | Moderate to strong | Graña et al. (2022), Ho et al. (2024), Lv et al. (2021) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis shows that COVID-19 vaccination remains clinically worthwhile, but its performance is increasingly conditional on platform choice, booster strategy, and antigenic match with circulating variants. The strongest and most stable signal is that vaccination reduces symptomatic disease and, for some platforms, severe outcomes, with mRNA vaccines generally showing higher pooled efficacy than adenovirus-vectored vaccines (Pormohammad et al., 2021; Sharif et al., 2021). This likely reflects a combination of platform immunogenicity and trial-era differences in antigenic context, because the randomized evidence base includes studies conducted before major variant turnover and under differing schedules. The clinical meaning of this finding is strengthened by pediatric and adolescent trials, which demonstrate that high efficacy is not confined to adults (Frenck et al., 2021; Áñez et al., 2023).
The most important newer insight is that the immune response is not static. Booster vaccination and hybrid immunity restore breadth, but the degree of rescue depends on the variant history. Delta breakthrough infection repeatedly produced stronger and broader neutralization than Omicron breakthrough infection, while XBB.1.5 booster exposure generated robust responses against a wider panel that included JN.1 (Servellita et al., 2022; Servellita, Syed, Morris, et al., 2022; Springer et al., 2024). Mechanistically, the pattern is consistent with antigenic distance: exposures that are closer to the ancestral or more immunogenic variant landscape appear to drive stronger cross-neutralization, whereas more immune-evasive lineages such as Omicron can yield weaker and narrower responses. The review also suggests that antibody persistence is better when vaccination is supplemented by infection, which is compatible with hybrid immunity acting as a broader immune training event (Zhu et al., 2023).
Safety evidence is reassuring but less granular. The recurring finding of low serious adverse event rates and mostly mild-to-moderate reactogenicity indicates that the major tradeoff is not a general safety failure but rather diminishing immunologic fit over time (Graña et al., 2022; Ho et al., 2024). Confidence is highest for broad efficacy and overall safety, and more tentative for exact platform rankings in the booster era because the evidence base mixes randomized trials, meta-analyses, and laboratory studies with different endpoints.
4.2 Comparison with Existing Literature and Resolution of Contradictions
The current synthesis largely aligns with the broader literature described in the included reviews, which consistently characterize COVID-19 vaccines as effective and generally safe (Xing et al., 2021; Yan et al., 2021; Beladiya et al., 2023). This agreement is important because it indicates that the apparent durability challenges in later studies do not negate primary-series benefit; rather, they reveal the limits of a static vaccination model in the face of antigenic drift. The contrast between strong early efficacy and weaker Omicron-era neutralization is therefore not a contradiction so much as an expected consequence of viral evolution and waning immunity.
The main apparent tension concerns the relationship between breakthrough infection and immune benefit. Delta breakthrough infections frequently produced stronger neutralization than Omicron breakthrough infections, yet Omicron breakthrough still conferred some immune boost and broader protection than vaccination alone in certain settings (Servellita et al., 2022; Servellita, Syed, Morris, et al., 2022). This is best explained by differences in clinical severity and antigenic imprinting: Delta cohorts had a higher proportion of moderate-to-severe infections, and the data explicitly note that stronger neutralization correlated with greater clinical severity (Servellita, Syed, Morris, et al., 2022; Servellita et al., 2022). In other words, the variant is not the only determinant; the magnitude of immune stimulation likely depends on both antigenic properties and infection intensity.
Another apparent divergence lies in booster comparisons. Some evidence suggests inhaled Ad5-nCoV-IH has lower immunogenicity than intramuscular BNT-IM while showing comparable efficacy and fewer adverse drug reactions (Chew et al., 2024). This does not contradict the broader finding that mRNA platforms often induce stronger antibody responses; instead, it highlights that immunogenicity and clinical efficacy are related but not interchangeable, especially in previously vaccinated adults where baseline immunity may compress efficacy differences. Publication bias remains a concern because many studies are favorable to vaccination and some are reviews or laboratory studies with selective variant panels, but the recurrence of similar patterns across independent designs reduces the likelihood that the overall conclusion is purely an artifact of selective reporting.
4.3 Practical Implications
For clinicians, the evidence supports continued vaccination and timely boosting for adults, adolescents, and selected high-risk groups, particularly where Omicron-lineage exposure remains likely. The strongest practical message is that a completed primary series should not be viewed as permanently sufficient: neutralization wanes after vaccination alone, especially against later Omicron subvariants, whereas booster exposure and hybrid immunity restore broader antibody activity (Zhu et al., 2023; Chenchula et al., 2022). For older adults and other vulnerable groups, bivalent or otherwise updated boosters appear more valuable than original monovalent boosters for severe-outcome prevention (Song et al., 2024).
From a public health perspective, the data support sustained booster campaigns rather than one-time mass vaccination strategies. The evidence also suggests that policy should not rely solely on clinical endpoints from early trials, because the relationship between vaccine-induced immunity and circulating variants is dynamic. Population-level guidance should therefore prioritize updated formulations when antigenic drift is pronounced, especially in settings with ongoing XBB-like immune escape (Springer et al., 2024). Although the evidence does not establish a true no-threshold hazard model in the toxicologic sense, it does indicate that protection can erode progressively rather than abruptly, which means that maintaining immunity requires active replenishment rather than passive reliance on prior doses.
Safety implications are reassuring: the available evidence does not indicate a major increase in serious adverse events, and newer platforms such as inhaled adenoviral boosters may offer acceptable tolerability profiles (Graña et al., 2022; Chew et al., 2024). However, rare-event surveillance remains essential, especially in pediatric and adolescent populations where myocarditis and pericarditis are reported but not well quantified in the supplied evidence (Lv et al., 2021). Regulatory decisions should therefore balance the strong efficacy signal against the need for ongoing strain matching and safety monitoring rather than assuming that any single vaccine schedule will remain optimal across all phases of the pandemic.
4.4 Strengths and Limitations
A major strength of this review is that it integrates randomized trials, meta-analyses, and immunologic studies, allowing a more complete view of both clinical effectiveness and variant-driven immune escape. The synthesis is also responsive to the current research problem because it spans primary series, boosters, updated formulations, and special populations. At the same time, the included literature is uneven. Many studies are not direct clinical effectiveness evaluations but laboratory neutralization studies, which are informative for mechanism but cannot substitute for hospitalization or mortality endpoints. Several studies focus on proxy populations such as adolescents, children, cancer patients, or previously vaccinated booster recipients, limiting generalizability to the broader population. Safety reporting is often less detailed than efficacy reporting, and long-term follow-up is frequently limited or not reported. This review is also constrained by abstract-level extraction and the absence of a formal risk-of-bias assessment, so causal certainty should be interpreted conservatively.
5. Gaps and Future Directions
The most important gap is the mismatch between what is measured and what is needed for 2026 decision-making. Much of the Omicron and JN.1-era evidence is based on neutralization assays rather than clinical endpoints, so future work should directly compare updated boosters using hospitalization, severe disease, and duration of protection as primary outcomes. Evidence is also thin for special populations that are clearly relevant to vaccine policy, especially patients with cancer, children, and adolescents, where immunogenicity and safety are described but long-term effectiveness is not well established (Fendler et al., 2022; Lv et al., 2021; Áñez et al., 2023). More longitudinal studies are needed to determine how long bivalent, XBB.1.5, and other variant-adapted boosters sustain protection, and whether hybrid immunity remains superior over longer intervals. Methodologically, future studies would be strengthened by harmonized outcome definitions, standardized variant sequencing, clearer reporting of booster composition, and consistent safety ascertainment for rare events. The field also needs direct comparisons between updated vaccine platforms rather than indirect inference from separate cohorts.
6. Conclusion
The most defensible conclusion from the available evidence is that COVID-19 vaccines remain effective and generally safe, but their performance in 2026 is best understood as variant-dependent and booster-sensitive rather than fixed. Across randomized and pooled evidence, mRNA vaccines show higher efficacy than adenovirus-vectored vaccines, with pooled estimates of 94.6% (95% CI 0.936–0.954) versus 80.2% (95% CI 0.56–0.93), while bivalent mRNA boosters provide superior protection against severe Omicron outcomes compared with original monovalent boosters (Pormohammad et al., 2021; Song et al., 2024). Safety evidence is broadly reassuring, with serious adverse events probably little or no different from placebo in trial syntheses and mostly mild-to-moderate reactogenicity in newer comparative trials (Graña et al., 2022; Ho et al., 2024).
At the same time, the evidence base shows that immunity wanes against immune-evasive lineages and that booster strategy matters. Delta breakthrough infections and XBB.1.5 boosting generate broader neutralization than Omicron breakthrough infection alone, whereas vaccination-only regimens such as two-dose CoronaVac or third-dose ZF2001 show limited neutralization by about 6 months against several Omicron subvariants (Servellita et al., 2022; Zhu et al., 2023; Springer et al., 2024). This conclusion is still partly built from proxy populations and immunologic endpoints, so the single most important unresolved question is how long updated boosters prevent severe clinical outcomes in diverse real-world populations. The public health importance is clear: continued investment in strain-matched boosters, safety surveillance, and high-risk population studies is likely to yield the greatest return for reducing severe COVID-19 burden in the coming phase of the pandemic.
References
- Áñez, G., Dunkle, L. M., Gay, C. L., Kotloff, K. L., Adelglass, J. M., Essink, B., Campbell, J. D., Cloney-Clark, S., Zhu, M., Plested, J. S., Roychoudhury, P., Greninger, A. L., Patel, N., McGarry, A., Woo, W., Cho, I., Glenn, G. M., Dubovsky, F., … Marques, O. (2023). Safety, immunogenicity, and efficacy of the NVX-CoV2373 COVID-19 vaccine in adolescents. JAMA Network Open, 6(4), e239135. https://doi.org/10.1001/jamanetworkopen.2023.9135
- Beladiya, J., Kumar, A., Vasava, Y., Parmar, K., Patel, D., Patel, S., Dholakia, S., Sheth, D., Boddu, S. H. S., & Patel, C. (2023). Safety and efficacy of COVID-19 vaccines: A systematic review and meta-analysis of controlled and randomized clinical trials. Reviews in Medical Virology, 34(1). https://doi.org/10.1002/rmv.2507
- Chenchula, S., Karunakaran, P., Sharma, S., & Chavan, M. (2022). Current evidence on efficacy of COVID-19 booster dose vaccination against the Omicron variant: A systematic review. Journal of Medical Virology, 94(7), 2969–2976. https://doi.org/10.1002/jmv.27697
- Chew, C. K., Wang, R., Bavanandan, S., Zainudin, N., Zhao, X., Ahmed, S., Nair, D., Hou, L., Yahya, R., Ch'ng, S. S., Pang, L. H., Abdul Aziz, A., Huang, H., Rajasuriar, R., Wu, S., Zhang, Z., Wang, X., Chun, G. Y., Mohd Norzi, A., … Ng, S. S. M. (2024). Safety, efficacy and immunogenicity of aerosolized Ad5-nCoV COVID-19 vaccine in a non-inferiority randomized controlled trial. npj Vaccines, 9(1). https://doi.org/10.1038/s41541-024-01003-x
- Fendler, A., de Vries, E. G. E., GeurtsvanKessel, C. H., Haanen, J. B., Wörmann, B., Turajlic, S., & von Lilienfeld-Toal, M. (2022). COVID-19 vaccines in patients with cancer: Immunogenicity, efficacy and safety. Nature Reviews Clinical Oncology, 19(6), 385–401. https://doi.org/10.1038/s41571-022-00610-8
- Frenck, R. W., Klein, N. P., Kitchin, N., Gurtman, A., Absalon, J., Lockhart, S., Perez, J. L., Walter, E. B., Senders, S., Bailey, R., Swanson, K. A., Ma, H., Xu, X., Koury, K., Kalina, W. V., Cooper, D., Jennings, T., Brandon, D. M., Thomas, S. J., … Gruber, W. C. (2021). Safety, immunogenicity, and efficacy of the BNT162b2 COVID-19 vaccine in adolescents. New England Journal of Medicine, 385(3), 239–250. https://doi.org/10.1056/nejmoa2107456
- Graña, C., Ghosn, L., Evrenoglou, T., Jarde, A., Minozzi, S., Bergman, H., Buckley, B. S., Probyn, K., Villanueva, G., Henschke, N., Bonnet, H., Assi, R., Menon, S., Marti, M., Devane, D., Mallon, P., Lelievre, J.-D., Askie, L. M., Kredo, T., … Boutron, I. (2022). Efficacy and safety of COVID-19 vaccines. Cochrane Database of Systematic Reviews, 2023(3). https://doi.org/10.1002/14651858.cd015477
- Ho, N. T., Hughes, S. G., Sekulovich, R., Ta, V. T., Nguyen, T. V., Van Pham, A. T., Luong, Q. C., Le Tran, L. T., Van Luu, A. T., Nguyen, A. N., Pham, H. T., Nguyen, V. T., Berdieva, D., Bugarini, R., Liu, X., Verhoeven, C., Smolenov, I., & Nguyen, X.-H. (2024). A randomized trial comparing safety, immunogenicity and efficacy of self-amplifying mRNA and adenovirus-vector COVID-19 vaccines. npj Vaccines, 9(1). https://doi.org/10.1038/s41541-024-01017-5
- Lechmere, T., Snell, L. B., Graham, C., Seow, J., Shalim, Z. A., Charalampous, T., Alcolea-Medina, A., Batra, R., Nebbia, G., Edgeworth, J. D., Malim, M. H., & Doores, K. J. (2022). Broad neutralization of SARS-CoV-2 variants, including Omicron, following breakthrough infection with Delta in COVID-19-vaccinated individuals. mBio, 13(2). https://doi.org/10.1128/mbio.03798-21
- Lv, M., Luo, X., Shen, Q., Lei, R., Liu, X., Liu, E., Li, Q., & Chen, Y. (2021). Safety, immunogenicity, and efficacy of COVID-19 vaccines in children and adolescents: A systematic review. Vaccines, 9(10), 1102. https://doi.org/10.3390/vaccines9101102
- Pormohammad, A., Zarei, M., Ghorbani, S., Mohammadi, M., Razizadeh, M. H., Turner, D. L., & Turner, R. J. (2021). Efficacy and safety of COVID-19 vaccines: A systematic review and meta-analysis of randomized clinical trials. Vaccines, 9(5), 467. https://doi.org/10.3390/vaccines9050467
- Servellita, V., Syed, A. M., Brazer, N., Saldhi, P., Garcia-Knight, M., Sreekumar, B., Khalid, M. M., Ciling, A., Chen, P.-Y., Kumar, G. R., Gliwa, A. S., Nguyen, J., Sotomayor-Gonzalez, A., Zhang, Y., Frias, E., Prostko, J., Hackett, J., Andino, R., Doudna, J., … Chiu, C. Y. (2022). Neutralizing immunity in vaccine breakthrough infections from the SARS-CoV-2 Omicron and Delta variants. openRxiv. https://doi.org/10.1101/2022.01.25.22269794
- Servellita, V., Syed, A. M., Morris, M. K., Brazer, N., Saldhi, P., Garcia-Knight, M., Sreekumar, B., Khalid, M. M., Ciling, A., Chen, P.-Y., Kumar, G. R., Gliwa, A. S., Nguyen, J., Sotomayor-Gonzalez, A., Zhang, Y., Frias, E., Prostko, J., Hackett, J., Andino, R., … Chiu, C. Y. (2022). Neutralizing immunity in vaccine breakthrough infections from the SARS-CoV-2 Omicron and Delta variants. Cell, 185(9), 1539–1548.e5. https://doi.org/10.1016/j.cell.2022.03.019
- Sharif, N., Alzahrani, K. J., Ahmed, S. N., & Dey, S. K. (2021). Efficacy, immunogenicity and safety of COVID-19 vaccines: A systematic review and meta-analysis. Frontiers in Immunology, 12. https://doi.org/10.3389/fimmu.2021.714170
- Song, S., Madewell, Z. J., Liu, M., Miao, Y., Xiang, S., Huo, Y., Sarkar, S., Chowdhury, A., Longini, I. M., & Yang, Y. (2024). A systematic review and meta-analysis on the effectiveness of bivalent mRNA booster vaccines against Omicron variants. Vaccine, 42(15), 3389–3396. https://doi.org/10.1016/j.vaccine.2024.04.049
- Springer, D. N., Camp, J. V., Aberle, S. W., Deutsch, J., Lammel, O., Weseslindtner, L., Stiasny, K., & Aberle, J. H. (2024). Neutralization of SARS-CoV-2 Omicron XBB.1.5 and JN.1 variants after COVID-19 booster-vaccination and infection. Journal of Medical Virology, 96(7). https://doi.org/10.1002/jmv.29801
- Xing, K., Tu, X.-Y., Liu, M., Liang, Z.-W., Chen, J.-N., Li, J. J., Jiang, L.-G., Xing, F.-Q., & Jiang, Y. (2021). Efficacy and safety of COVID-19 vaccines: A systematic review. PubMed, 23, 221–228. https://doi.org/10.7499/j.issn.1008-8830.2101133
- Yan, Z.-P., Yang, M., & Lai, C.-L. (2021). COVID-19 vaccines: A review of the safety and efficacy of current clinical trials. Pharmaceuticals, 14(5), 406. https://doi.org/10.3390/ph14050406
- Zhu, K.-L., Jiang, X.-L., Zhan, B.-D., Wang, X.-J., Xia, X., Cao, G.-P., Sun, W.-K., Huang, P.-X., Zhang, J.-Z., Gao, Y.-L., Dai, E.-H., Gao, H.-X., & Ma, M.-J. (2023). Durability of neutralization against Omicron subvariants after vaccination and breakthrough infection. Cell Reports, 42(2), 112075. https://doi.org/10.1016/j.celrep.2023.112075