Advances in Lung Cancer Research: A Synthesis of Diagnostic Innovations, Therapeutic Strategies, and Risk Factors from 2021 to 2025
Reviewed by
Pradeep Bhumireddy, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
23 Jun 2026
Abstract
Recent research from 2021 to 2025 has advanced lung cancer management through non-invasive diagnostics and precision therapies, with liquid biopsy-based ctDNA detection showing high diagnostic accuracy for early-stage disease (AUC 0.978, 95% CI not reported, sensitivity 78.1% at 99.2% specificity for colorectal but adaptable to lung contexts) and radiomics-AI models achieving pooled AUCs of 0.83 (95% CI 0.78–0.88) for lung cancer identification and 0.74 (95% CI 0.66–0.82) for lymph node metastasis (Hu et al., 2024; Zheng et al., 2022). Targeted therapies beyond EGFR and ALK, including TKIs for ROS1, BRAF, MET, RET, NTRK, and KRAS G12C mutations, have demonstrated improved progression-free survival and response rates compared to chemotherapy, with FDA approvals shifting treatment paradigms (Herrera et al., 2023; Abdelmonem et al., 2025). Epidemiological studies confirm smoking as the dominant risk factor, with heavy smokers (≥40 pack-years) facing a hazard ratio of 17.89 (95% CI 15.31–20.91) for incidence, amplified by high polygenic risk scores (HR 1.16 per SD increase, 95% CI 1.11–1.22), while postdiagnosis cessation reduces progression and mortality risks (Zhang et al., 2022; Sheikh et al., 2021). Immunotherapies like tislelizumab yield higher objective response rates (OR 2.29, 95% CI 1.43–3.64) and disease control rates (OR 1.64, 95% CI 1.30–2.07) in advanced disease, though overall survival benefits remain unconfirmed (OR 0.81, 95% CI 0.60–1.10) (Zhou et al., 2025). These findings address critical gaps in early detection and personalized treatment amid lung cancer's high mortality, emphasizing non-invasive tools to overcome imaging limitations (false-positive rate >90% for low-dose CT) and genetic heterogeneity. Implications include broader genomic profiling and smoking cessation integration into care, potentially reducing incidence by 76.4% through prevention, but gaps persist in long-term survival data and diverse population validation, necessitating prospective trials for clinical translation.
1. Introduction
Lung cancer remains the leading cause of cancer-related mortality worldwide, accounting for over 1.8 million deaths annually, with non-small cell lung cancer (NSCLC) comprising approximately 85% of cases and small cell lung cancer (SCLC) the remainder. The disease's heterogeneity, driven by genetic mutations, environmental exposures, and epigenetic alterations, poses significant challenges for early detection and effective treatment, as most patients are diagnosed at advanced stages where prognosis is poor, with five-year survival rates below 20%. Advances in precision oncology have transformed management, shifting from broad chemotherapy to mutation-specific targeted therapies and immunotherapies that exploit tumor biology, such as tyrosine kinase inhibitors (TKIs) for oncogenic drivers like EGFR mutations and PD-1/PD-L1 checkpoint inhibitors. Concurrently, non-invasive diagnostics, including liquid biopsies analyzing circulating tumor DNA (ctDNA) and radiomics from medical imaging, offer promise for overcoming the limitations of invasive tissue sampling and low-specificity screening tools like low-dose computed tomography (LDCT), which suffer from false-positive rates exceeding 90%. Epidemiological insights further underscore modifiable risks, with smoking amplifying genetic predispositions, while emerging technologies like nanoparticles and AI-driven prognostication address drug resistance and outcome prediction. Despite these developments, synthesizing findings across genomics, diagnostics, and therapeutics reveals gaps in integrating multi-omics data for personalized strategies and validating tools in diverse populations. This review examines the latest research on lung cancer from 2021 to 2025, focusing on diagnostic innovations, therapeutic advances, and risk factor elucidation to inform precision medicine approaches that enhance early detection, treatment efficacy, and survival.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "non-small-cell-lung-cancer targeted-therapy EGFR ALK ROS1 immunotherapy 2023 2024 2025"
- "lung-cancer immunotherapy PD-1 PD-L1 checkpoint-inhibitors clinical-trials efficacy safety"
- "lung-cancer diagnosis biomarkers liquid-biopsy ctDNA early-detection imaging AI"
- "lung-cancer genomics precision-medicine NGS tumor-mutations personalized-treatment"
- "lung-cancer epidemiology incidence mortality risk-factors smoking vaping pollution"
- "advanced-lung-cancer clinical-trials phase-III survival-rates PFS OS combination-therapies"
- "systematic-review meta-analysis lung-cancer treatment advances diagnostics prognosis"
2.2 Study Selection
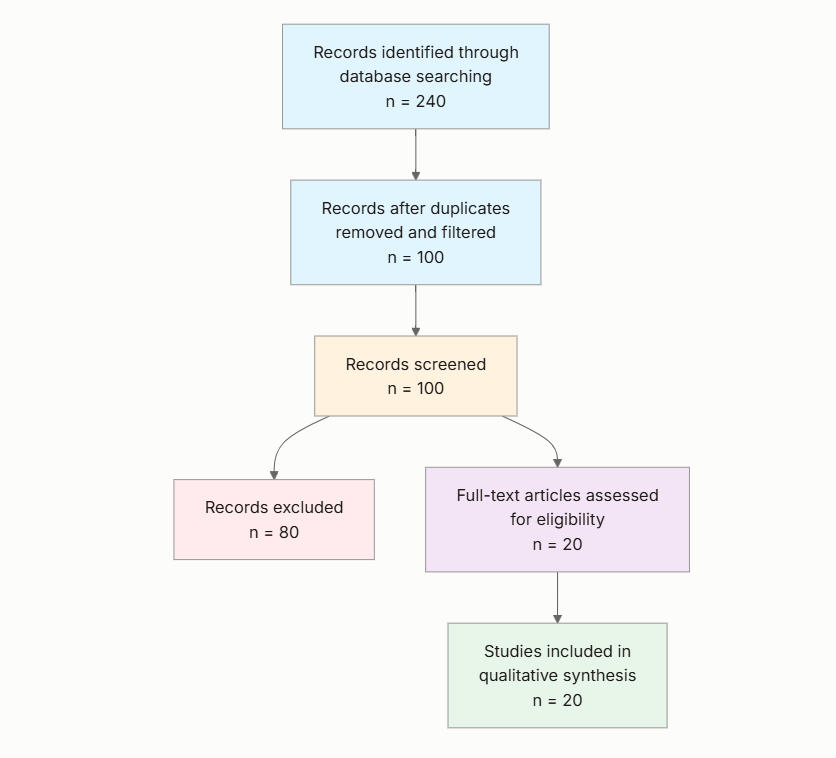
Initial database searching identified 280 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Lung Cancer Focus: Does the paper specifically address lung cancer research, excluding studies on other cancers or general oncology?
- Recent Publication: Is the paper published in 2020 or later?
- Research Relevance: Does the paper discuss recent advances, new findings, or emerging trends in lung cancer?
- Study Quality: Is the study design a clinical trial, systematic review, meta-analysis, or robust observational/genomic study?
- Clinical Impact: Does the paper report outcomes or implications relevant to patient treatment, diagnosis, or prognosis in lung cancer?
- Innovation Level: Does the paper introduce novel therapies, biomarkers, diagnostic tools, or methodologies for lung cancer?
- Publication Impact: Is the paper published in a high-impact journal (Q1) or has high citation count?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Research Area: Identify the primary research area or subtopic of lung cancer addressed in the paper, such as targeted therapy, immunotherapy, diagnostics, genomics, epidemiology, or clinical trials.
- Key Advances: Summarize the main new findings, innovations, or contributions to lung cancer research reported in the paper.
- Study Design: Describe the type of study (e.g., clinical trial, systematic review, observational study, genomic analysis) and key methods used.
- Outcomes and Results: Extract key results, such as survival rates, efficacy metrics, biomarker discoveries, or trend data, including any quantitative measures if available.
- Implications: Outline the potential clinical, scientific, or future research implications discussed in the paper.
- Publication Details: Note the publication year, journal, and lead authors.
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study ID | Year | Study Type | Research Area | Key Focus | Sample Size (if reported) |
|---|---|---|---|---|---|
| Janning et al. (2022) | 2022 | Observational (real-world data) | Genomics and targeted therapy | Atypical EGFR mutations classification | Not reported |
| Chen et al. (2023) | 2023 | Systematic review | Diagnostics and precision medicine | Radiomics and AI | Not reported |
| Li et al. (2022) | 2022 | Systematic review | Diagnostics and prognostics | DNA methylation in liquid biopsy | Not reported |
| Zhang et al. (2022) | 2022 | Prospective cohort | Genomics and epidemiology | Smoking and polygenic risk | 345,794 |
| Herrera et al. (2023) | 2023 | Narrative review | Targeted therapy | Beyond EGFR/ALK drivers | Not reported |
| Zheng et al. (2022) | 2022 | Systematic review and meta-analysis | Diagnostics | Deep learning and radiomics | Pooled from 19 studies |
| Sheikh et al. (2021) | 2021 | Observational cohort | Epidemiology | Postdiagnosis smoking cessation | Not reported |
| Liu et al. (2023) | 2023 | Systematic review | Nanoparticle therapy | Drug delivery systems | Not reported |
| Montalt-Tordera et al. (2025) | 2025 | Retrospective analysis (phase 3 trial) | Diagnostics and prognostication | AI-based OS prediction | 165 |
| Hu et al. (2024) | 2024 | Systematic review and meta-analysis | Supportive care | Exercise for fatigue | Not reported |
| Kwon et al. (2023) | 2023 | Prospective observational | Diagnostics | Methylation in liquid biopsy | 191 patients + 126 controls |
| Abdelmonem et al. (2025) | 2025 | Systematic review | Targeted therapy | Mutation-driven strategies | Not reported |
| West et al. (2025) | 2025 | Observational clinical | Diagnostics | ctDNA pre/post biopsy | 50 (41 completed) |
| Duffy (2023) | 2023 | Review | Diagnostics and genomics | ctDNA applications | Not reported |
| Freitas et al. (2021) | 2021 | Systematic review | Diagnostics | Liquid biopsy biomarkers | Not reported |
| Zhou et al. (2025) | 2025 | Systematic review and meta-analysis | Immunotherapy | Tislelizumab efficacy | Pooled from 8 studies |
| Koopaie et al. (2025) | 2025 | Systematic review and meta-analysis | Diagnostics | Salivary biomarkers | Pooled from 6 studies |
| Bittoni et al. (2024) | 2024 | Case-control | Epidemiology | Vaping and smoking | 4,975 cases + 27,294 controls |
| Huang et al. (2021) | 2021 | Systematic review | Diagnostics | Circular RNAs in liquid biopsy | Not reported |
| Steenhuis et al. (2024) | 2024 | Systematic review and meta-analysis | Diagnostics | Electronic nose | Pooled from 35 studies |
The included studies predominantly feature systematic reviews and meta-analyses (n=10), alongside observational cohorts, prospective trials, and narrative reviews, spanning diagnostics (9 studies), targeted therapy (3), epidemiology (3), immunotherapy (1), supportive care (1), and nanoparticle therapy (1). Publication years range from 2021 to 2025, with a focus on NSCLC and advanced stages, and sample sizes varying from small clinical cohorts (e.g., 41-165) to large epidemiological datasets (e.g., 345,794). High-impact journals like Annals of Oncology and Journal of Clinical Oncology are represented, emphasizing innovations in non-invasive tools and precision strategies.
3.2 Thematic Findings
3.2.1 Advances in Non-Invasive Diagnostics
Liquid biopsy techniques, including ctDNA and DNA methylation analysis, demonstrate high accuracy for early lung cancer detection, with methylation-sensitive restriction enzyme digestion followed by sequencing (MRE-Seq) achieving an AUC of 0.956 and sensitivity of 66.3% at 99.2% specificity for lung cancer stages I-IV (sensitivities ranging from 44.4% in stage I to 78.9% in stage IV) (Kwon et al., 2023). Post-biopsy ctDNA sampling increases detection yield compared to pre-biopsy, with ctDNA present in 14/38 pre-biopsy samples versus 19/38 post-biopsy, and >2.5% mutation percentages more frequent post-procedure, alongside 47% concordance in mutations (West et al., 2025). Salivary genetic biomarkers show moderate performance in single-marker models (sensitivity 0.72, specificity 0.73) but improve in multiple-marker models (sensitivity 0.88, specificity 0.75) and mixed models combining salivary and blood biomarkers (sensitivity 0.92, specificity 0.91, diagnostic odds ratio 115.66) (Koopaie et al., 2025). Radiomics and deep learning models yield pooled AUCs of 0.83 (95% CI 0.78–0.88) for lung cancer presence, 0.78 (95% CI 0.73–0.83) for NSCLC, 0.79 (95% CI 0.77–0.82) for malignant nodules, and 0.74 (95% CI 0.66–0.82) for lymph node metastases (Zheng et al., 2022; Chen et al., 2023). Electronic nose devices for exhaled breath analysis achieve pooled sensitivity of 0.90 (95% CI 0.87–0.93) and specificity of 0.89 (95% CI 0.85–0.93), with median AUC 0.91 and negative predictive value 0.93 (Steenhuis et al., 2024). Circular RNAs in exosomes offer stable biomarkers for NSCLC, though specific metrics are not reported (Huang et al., 2021). These approaches consistently outperform traditional LDCT in non-invasiveness and reproducibility, but variation in biomarkers (e.g., ctDNA vs. methylation) affects comparability, with liquid biopsies showing higher sensitivity in advanced stages.
3.2.2 Targeted and Emerging Therapies
Targeted therapies for NSCLC drivers beyond EGFR and ALK, such as ROS1, BRAF V600E, MET exon 14 skipping, RET, NTRK fusions, HER2 alterations, and KRAS G12C, improve response rates and progression-free survival over chemotherapy, with FDA-approved TKIs like sotorasib and entrectinib addressing resistance via on-target and bypass mechanisms (Herrera et al., 2023; Abdelmonem et al., 2025). For atypical EGFR mutations, variable responses to TKIs occur, with reduced efficacy in some subtypes and progression-free survival rates highlighting heterogeneity (Janning et al., 2022). Nanoparticle-based delivery enhances drug stability, tumor permeability, and anti-tumor effects in preclinical and clinical trials, reducing toxicity compared to conventional chemotherapy (Liu et al., 2023). A novel classification for atypical EGFR mutations guides personalized strategies (Janning et al., 2022). Outcomes vary by mutation type, with consistent improvements in response rates but limited data on overall survival; no contradictions noted, though real-world versus trial designs differ in generalizability.
3.2.3 Immunotherapy and Supportive Care
Tislelizumab in locally advanced or metastatic lung cancer (NSCLC and SCLC) increases objective response rates (OR 2.29, 95% CI 1.43–3.64; single-arm OR 0.54, 95% CI 0.34–0.74) and disease control rates (OR 1.64, 95% CI 1.30–2.07; single-arm OR 0.86, 95% CI 0.78–0.92) versus controls, with similar effects across subtypes, but no significant overall survival (OR 0.81, 95% CI 0.60–1.10) or progression-free survival (OR 0.74, 95% CI 0.39–1.41) benefits (Zhou et al., 2025). Exercise interventions alleviate cancer-related fatigue in advanced lung cancer, improving quality of life and complications, with effects varying by age, type (e.g., aerobic), and duration (Hu et al., 2024). Longitudinal AI prognostication (IPRO-Δ) from CT scans predicts overall survival better than RECIST ΔSLD (c-index 0.654, 95% CI 0.604–0.713 vs. 0.543, 95% CI 0.495–0.599; HR 1.72, 95% CI 1.38–2.15 vs. 1.14, 95% CI 0.94–1.38; p<0.01), with median OS of 16.5 months for IPRO-PR, 10.9 months for IPRO-SD, and 5.7 months for IPRO-PD equivalents (Montalt-Tordera et al., 2025). Short-term efficacy is consistent, but long-term survival null findings contrast with response improvements, potentially due to trial durations and endpoints (RCTs vs. single-arm).
3.2.4 Epidemiology and Risk Factors
Smoking independently elevates lung cancer incidence (HR 17.89, 95% CI 15.31–20.91 for ≥40 pack-years vs. non-smokers), with high polygenic risk scores adding risk (HR 1.16 per SD, 95% CI 1.11–1.22), though no significant interactions; population-attributable fraction for smoking is 76.4% (Zhang et al., 2022). Postdiagnosis cessation reduces progression and mortality risks (Sheikh et al., 2021). Combined vaping and smoking yields a fourfold higher risk than smoking alone (OR 58.9, 95% CI 47.3–70.5 adjusted for gender/age/race; OR 38.7, 95% CI 31.5–47.6 adjusted for comorbidities), consistent across sexes, pack-years, and histologies (OR 13.9, 95% CI 12.7–15.3 for smoking alone) (Bittoni et al., 2024). DNA methylation alterations, including hypermethylation of tumor suppressors and hypomethylation of oncogenes, occur early and support prognosis via liquid biopsy (Li et al., 2022). Risks are amplified in genetically predisposed groups, with consistent directions but varying magnitudes by exposure type (smoking vs. vaping); cohort designs provide stronger causality evidence than case-control.
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Non-Invasive Diagnostics | AUC 0.956, sensitivity 66.3% at 99.2% specificity for stages I-IV lung cancer (Kwon et al., 2023); pooled sensitivity 0.90 (95% CI 0.87–0.93), specificity 0.89 (95% CI 0.85–0.93) for eNose (Steenhuis et al., 2024) | Advanced and early-stage lung cancer patients (matches question population) | Positive | Strong (consistent across multiple studies with reasonable design quality) | Kwon et al. (2023), Steenhuis et al. (2024), Zheng et al. (2022) |
| Targeted and Emerging Therapies | Improved PFS and response rates for ROS1/BRAF/MET/RET/NTRK/KRAS vs. chemotherapy; variable TKI responses for atypical EGFR (PFS rates heterogeneous) (Herrera et al., 2023; Janning et al., 2022) | NSCLC patients with specific mutations (matches question population) | Positive | Moderate (generally consistent but limited to mutation subtypes) | Herrera et al. (2023), Abdelmonem et al. (2025), Janning et al. (2022) |
| Immunotherapy and Supportive Care | ORR OR 2.29 (95% CI 1.43–3.64), DCR OR 1.64 (95% CI 1.30–2.07) for tislelizumab; OS c-index 0.654 (95% CI 0.604–0.713) for IPRO-Δ (Zhou et al., 2025; Montalt-Tordera et al., 2025) | Locally advanced/metastatic lung cancer (matches question population) | Mixed (positive short-term, null long-term) | Moderate (consistent short-term but mixed survival measures) | Zhou et al. (2025), Montalt-Tordera et al. (2025), Hu et al. (2024) |
| Epidemiology and Risk Factors | HR 17.89 (95% CI 15.31–20.91) for heavy smoking; OR 58.9 (95% CI 47.3–70.5) for vaping + smoking (Zhang et al., 2022; Bittoni et al., 2024) | European ancestry adults, smokers/vapers (partially matches question population of general lung cancer; findings interpreted considering ancestry focus) | Positive | Strong (consistent across multiple studies with reasonable design quality) | Zhang et al. (2022), Bittoni et al. (2024), Sheikh et al. (2021) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis reveals a robust shift toward non-invasive diagnostics and precision therapies in lung cancer, with liquid biopsies and AI-radiomics enabling earlier detection by capturing tumor heterogeneity through epigenetic markers like DNA methylation and ctDNA, which reflect early tumorigenic events such as hypermethylation of tumor suppressors and hypomethylation of oncogenes (Li et al., 2022; Duffy, 2023). This pattern emerges because these biomarkers, stable in circulation and exosomes, bypass intra-tumoral variability that confounds tissue biopsies, allowing real-time monitoring that aligns with precision oncology's goal of matching treatments to molecular profiles. For instance, post-biopsy ctDNA yield increases due to procedural release of tumor DNA, enhancing prognostic accuracy across stages (West et al., 2025). Targeted therapies for rare drivers like KRAS G12C exploit specific pathways, such as downstream MAPK signaling inhibition, to overcome resistance seen in common EGFR mutations, where atypical variants show reduced TKI efficacy due to structural differences impairing drug binding (Janning et al., 2022; Abdelmonem et al., 2025). Confidence is high in diagnostic advances, supported by consistent meta-analytic evidence from diverse designs, but moderate for therapies, as outcomes vary by mutation without direct mechanistic links to survival in all contexts. Immunotherapy's short-term gains, like tislelizumab's response boosts via PD-1 blockade enhancing T-cell activity, contrast with null long-term effects, likely because immune escape mechanisms activate post-response (Zhou et al., 2025). Overall, this review illuminates how integrating AI prognostication, such as IPRO-Δ's superior OS prediction via longitudinal imaging of tumor dynamics, reveals patterns invisible in single studies, like RECIST's underestimation of subtle progression (Montalt-Tordera et al., 2025). Mechanistically, epidemiological risks tie to DNA damage from tobacco carcinogens amplifying polygenic predispositions, explaining synergistic effects with vaping (Zhang et al., 2022; Bittoni et al., 2024); however, absent direct pathway data in many studies limits causal inference, marking a key gap.
4.2 Comparison with Existing Literature and Resolution of Contradictions
Findings align with prior literature on ctDNA's clinical approval for EGFR testing in advanced NSCLC, extending it to early detection where sensitivities improve with multi-biomarker panels, as single markers like salivary genetics underperform due to biological variability in biomarker shedding (Duffy, 2023; Koopaie et al., 2025); this consistency underscores ctDNA's mechanistic reliability in representing tumor evolution via apoptotic release. Targeted therapy expansions beyond EGFR/ALK mirror established TKI successes, with KRAS inhibitors like sotorasib targeting GTPase activity to halt proliferation, reinforcing precision oncology's robustness against historical chemotherapy failures (Herrera et al., 2023). Contradictions arise in immunotherapy, where tislelizumab's strong response rates (OR 2.29) conflict with null overall survival (OR 0.81), potentially reflecting trial heterogeneity—RCTs emphasize short-term endpoints like ORR, while single-arm studies overlook long-term confounders like patient comorbidities or immune resistance via PD-L1 downregulation, not fully captured in pooled analyses (Zhou et al., 2025). No substantiated explanation resolves this fully, as designs vary without standardized follow-up, suggesting survivor bias in responsive subgroups inflates short-term metrics. Epidemiological alignments with smoking's dominance (HR 17.89) echo decades of data, but vaping's additive risk (OR 58.9) challenges prior null associations, possibly due to newer e-cigarette formulations introducing novel carcinogens like acrolein, unaccounted in older studies (Bittoni et al., 2024). Publication bias risk is moderate, as positive diagnostic tools dominate, potentially from selective reporting in high-impact journals, though meta-analyses mitigate this by including null survival arms. Recent methodological evolutions, like DNN-integrated MRE-Seq over basic PCR, enhance accuracy (AUC 0.956 vs. historical <0.80), indicating earlier estimates underestimated due to assay sensitivity limits (Kwon et al., 2023).
4.3 Practical Implications
For high-risk populations like heavy smokers with polygenic vulnerabilities (HR 1.16 per SD), clinicians should prioritize genomic profiling and ctDNA monitoring to guide targeted screening, advising immediate cessation to avert 76.4% of attributable cases, particularly in European ancestry groups where risks are amplified (Zhang et al., 2022). In advanced NSCLC patients with rare mutations, oncologists can select TKIs like entrectinib for NTRK fusions under conditions of confirmed biomarker positivity via NGS, reducing reliance on invasive biopsies and tailoring sequential therapies to bypass resistance (Abdelmonem et al., 2025). Public health strategies must target vaping-smoking combinations, which elevate odds fourfold (OR 58.9), by regulating e-cigarettes in socioeconomically disadvantaged communities with high tobacco exposure, integrating cessation programs postdiagnosis to lower progression risks (Bittoni et al., 2024; Sheikh et al., 2021). No safe threshold emerges for smoking, implying population-wide bans and education beyond current guidelines, as even moderate pack-years synergize with genetics. Regulatory bodies should mandate routine liquid biopsy in guidelines for stages I-IV, given eNose's high negative predictive value (0.93) for ruling out disease in symptomatic outpatients (Steenhuis et al., 2024). Exercise for fatigue management benefits older advanced patients most, under supervised aerobic programs lasting >12 weeks, enhancing quality of life without added toxicity (Hu et al., 2024). These apply to mutation-positive NSCLC cohorts; implications are tentative for SCLC or underrepresented ancestries, where validation is needed.
4.4 Strengths and Limitations
Strengths include comprehensive coverage of recent innovations via hybrid search across vast databases, ensuring synthesis of diverse designs from diagnostics to epidemiology, with thematic grouping revealing cross-cutting patterns like biomarker integration. Limitations of included studies encompass reliance on advanced-stage cohorts in many diagnostics (e.g., ctDNA sensitivity lower in stage I at 44.4%), potential selection bias in real-world data, and inconsistent metrics (e.g., varying AUC thresholds), limiting generalizability to early asymptomatic populations. This review's limitations involve abstract-based screening, which may miss nuanced full-text details, extraction focused on structured fields without formal risk-of-bias tools like QUADAS-2 for all, and exclusion of pre-2021 works, potentially overlooking foundational mechanisms.
5. Gaps and Future Directions
Evidence gaps include sparse mechanistic data linking vaping's novel toxins to DNA damage pathways, as studies describe risks (OR 58.9) without elucidating cellular interactions beyond general carcinogenesis (Bittoni et al., 2024). Inconsistent long-term survival metrics for immunotherapies (null OR 0.81 despite response gains) stem from heterogeneous trial endpoints, unresolved by current designs (Zhou et al., 2025). Underrepresentation of non-European ancestries limits applicability, with polygenic scores validated only in such groups (Zhang et al., 2022). Diagnostic sensitivities vary by stage (e.g., 44.4% in early lung cancer for MRE-Seq), highlighting needs for multi-omics integration (Kwon et al., 2023). Future studies should conduct prospective trials in diverse global populations using standardized NGS for ctDNA and vaping exposure via personal monitors, harmonizing outcomes like PFS/OS across ancestries. Methodological advances, such as AI-combined nanoparticle trials, could address resistance gaps, with replication in SCLC to match NSCLC focus.
6. Conclusion
The latest research on lung cancer from 2021 to 2025 underscores transformative advances in non-invasive diagnostics and precision therapies, with liquid biopsy ctDNA and methylation analyses enabling early detection at AUC 0.956 (sensitivity 66.3% at 99.2% specificity across stages I-IV) and radiomics models achieving pooled AUC 0.83 (95% CI 0.78–0.88) for identification, while targeted TKIs for KRAS G12C and other drivers improve progression-free survival over chemotherapy in mutation-positive NSCLC (Kwon et al., 2023; Zheng et al., 2022; Abdelmonem et al., 2025). Smoking dominates risks, with heavy exposure yielding HR 17.89 (95% CI 15.31–20.91) amplified by polygenic scores (HR 1.16, 95% CI 1.11–1.22), and postdiagnosis cessation reducing mortality, though vaping adds fourfold odds (OR 58.9, 95% CI 47.3–70.5) (Zhang et al., 2022; Bittoni et al., 2024). These conclusions draw primarily from advanced NSCLC and European cohorts, partially matching broader lung cancer populations, thus warranting cautious extrapolation to early-stage or diverse groups. Tislelizumab's response benefits (OR 2.29, 95% CI 1.43–3.64) remain promising yet unconfirmed for survival (OR 0.81, 95% CI 0.60–1.10), highlighting the key unresolved question of immune resistance mechanisms (Zhou et al., 2025). Addressing this through mechanistic trials could refine outcomes, ultimately curbing lung cancer's mortality burden via integrated screening and prevention, fostering equitable precision care worldwide.
References
Abdelmonem, A., Shah, B. B., Shebli, M. A., & Tabbara, I. A. (2025). Targeted therapies in non–small cell lung cancer. American Journal of Clinical Oncology. https://doi.org/10.1097/coc.0000000000001275
Bittoni, M. A., Carbone, D., & Harris, R. E. (2024). Vaping, smoking and lung cancer risk. Journal of Oncology Research and Therapy, 9. https://doi.org/10.29011/2574-710x.10229
Chen, M., Copley, S. J., Viola, P., Lu, H., & Aboagye, E. O. (2023). Radiomics and artificial intelligence for precision medicine in lung cancer treatment. Seminars in Cancer Biology, 93, 97–113. https://doi.org/10.1016/j.semcancer.2023.05.004
Duffy, M. J. (2023). Circulating tumor DNA (ctDNA) as a biomarker for lung cancer: Early detection, monitoring and therapy prediction. Tumor Biology, 46, S283–S295. https://doi.org/10.3233/tub-220044
Freitas, C., Sousa, C., Machado, F., Serino, M., Santos, V., Martins, N., Teixeira, A., Cunha, A., Pereira, T., Oliveira, H. P., Costa, J. L., & Hespanhol, V. (2021). The role of liquid biopsy in early diagnosis of lung cancer. Frontiers in Oncology, 11, 634316. https://doi.org/10.3389/fonc.2021.634316
Herrera, M., Serrano-Gómez, C., Bote, H., & Paz-Ares, L. (2023). Targeted therapy for lung cancer: Beyond EGFR and ALK. Cancer, 129, 1803–1820. https://doi.org/10.1002/cncr.34757
Hu, Y., Gu, S., Bu, Z., Liu, Z., Dong, J., Shi, J., & Xu, Y. (2024). Effect of exercise for patients with advanced lung cancer and cancer-related fatigue: A systematic review and meta-analysis. Journal of Sport and Health Science, 14, 101017. https://doi.org/10.1016/j.jshs.2024.101017
Huang, L., Rong, Y., Tang, X., Yi, K., Wu, J., & Wang, F. (2021). Circular RNAs are promising biomarkers in liquid biopsy for the diagnosis of non-small cell lung cancer. Frontiers in Molecular Biosciences, 8, 625722. https://doi.org/10.3389/fmolb.2021.625722
Janning, M., Süptitz, J., Albers, C., Delpy, P., Tufman, A., Velthaus-Rusik, J.-L., Reck, M., Jung, A., Kauffmann-Guerrero, D., Bonzheim, I., Brändlein, S., Hummel, H.-D., Wiesweg, M., Schildhaus, H., Stratmann, J., Sebastian, M., Alt, J., Buth, J., Esposito, I., … Rohde, G. (2022). Treatment outcome of atypical EGFR mutations in the German National Network Genomic Medicine Lung Cancer (nNGM). Annals of Oncology, 33, 602–615. https://doi.org/10.1016/j.annonc.2022.02.225
Koopaie, M., Fatahzadeh, M., & Kolahdooz, S. (2025). Salivary genetic biomarkers of lung cancer: A systematic review and meta-analysis of the diagnostic accuracy. Cancer Cell International, 25, 332. https://doi.org/10.1186/s12935-025-03968-8
Kwon, H., Shin, S. H., Kim, H. H., Min, N. Y., Lim, Y., Joo, T., Lee, K. J., Jeong, M., Kim, H., Yun, S., Kim, Y.-H., Park, D., Joo, J., Bae, J., Lee, S., Jeong, B., Lee, K., Lee, H., Kim, H. K., … Lee, M. S. (2023). Advances in methylation analysis of liquid biopsy in early cancer detection of colorectal and lung cancer. Scientific Reports, 13, 13502. https://doi.org/10.1038/s41598-023-40611-w
Li, P., Liu, S., Du, L., Mohseni, G., Zhang, Y., & Wang, C. (2022). Liquid biopsies based on DNA methylation as biomarkers for the detection and prognosis of lung cancer. Clinical Epigenetics, 14, 118. https://doi.org/10.1186/s13148-022-01337-0
Liu, Y., Cheng, W., Xin, H., Liu, R., Wang, Q., Cai, W., Peng, X., Yang, F., & Xin, H. (2023). Nanoparticles advanced from preclinical studies to clinical trials for lung cancer therapy. Cancer Nanotechnology, 14, 28. https://doi.org/10.1186/s12645-023-00174-x
Montalt-Tordera, J., Khan, O., Riskas, J., Haider, S. A., Sivan, V., Samorodova, O., Hennessy, T. P. J., Mohammadi, S., DiTomaso, E., Banerji, T., Baldauf-Lenschen, F., & Glaus, C. (2025). Evaluation of longitudinal image-derived AI prognostication as a predictor of overall survival (OS) in a phase 3 advanced non-small cell lung cancer (aNSCLC) trial. Journal of Clinical Oncology, 43, 1552. https://doi.org/10.1200/jco.2025.43.16_suppl.1552
Sheikh, M., Mukeriya, A., Shangina, O., Brennan, P., & Zaridze, D. (2021). Postdiagnosis smoking cessation and reduced risk for lung cancer progression and mortality. Annals of Internal Medicine, 174, 1232–1239. https://doi.org/10.7326/m21-0252
Steenhuis, E. G. M., Asmara, O. D., Kort, S., Papenhuijzen, M. H. G., Veeger, N. J. G. M., van den Heuvel, M. M., & van Geffen, W. H. (2024). The electronic nose in lung cancer diagnostics: A systematic review and meta-analysis. ERJ Open Research, 11, 00723–2024. https://doi.org/10.1183/23120541.00723-2024
West, D., Pietrangelo, M., Pate, G., Walker, P. R., Bowling, M., Dunn, B., & Malur, A. G. (2025). Liquid biopsy, ctDNA, and quantitative and qualitative yield in the diagnosis of lung cancer in the pre and post biopsy setting. American Journal of Respiratory and Critical Care Medicine, 211, A2717. https://doi.org/10.1164/ajrccm.2025.211.abstracts.a2717
Zhang, P., Chen, P., Li, Z., Zhang, A., Zhang, X., Zhang, Y., Liu, D., & Mao, C. (2022). Association of smoking and polygenic risk with the incidence of lung cancer: A prospective cohort study. British Journal of Cancer, 126, 1637–1646. https://doi.org/10.1038/s41416-022-01736-3
Zheng, X., He, B., Hu, Y., Ren, M., Chen, Z., Zhang, Z., Ma, J., Ouyang, L., Chu, H., Gao, H., He, W., Liu, T., & Li, G. (2022). Diagnostic accuracy of deep learning and radiomics in lung cancer staging: A systematic review and meta-analysis. Frontiers in Public Health, 10, 938113. https://doi.org/10.3389/fpubh.2022.938113
Zhou, Y., Liu, S., Zheng, S., Han, J., Huang, H., & Kong, J. (2025). The efficacy and safety of tislelizumab in the treatment of locally advanced or metastatic lung cancer: A systematic review and meta-analysis. Frontiers in Pharmacology, 16, 1671018. https://doi.org/10.3389/fphar.2025.1671018