Latest Research on Mental Health 2026: Trends and Treatments in Depression and Anxiety – A Synthesis of Global Findings from 2020-2026
Reviewed by
Shaantanu Kulkarni, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
22 Jun 2026
Abstract
Combined psychotherapy and pharmacotherapy emerges as the most effective approach for treating adult depression, outperforming either monotherapy alone with relative risks for treatment response of 1.27 (95% CI: 1.14-1.39) versus psychotherapy alone and 1.25 (95% CI: 1.14-1.37) versus pharmacotherapy alone, alongside improved remission rates of 1.23 (95% CI: 1.05-1.45) and greater acceptability compared to pharmacotherapy (RR=1.17; 95% CI: 1.02-1.32) (Cuijpers et al., 2020). Sequential integration of psychotherapy following initial pharmacotherapy response further reduces relapse risk in recurrent major depressive disorder, with consistent benefits across patient characteristics (Čihařová et al., 2026; Guidi & Fava, 2020). For anxiety disorders, selective serotonin reuptake inhibitors (SSRIs) and serotonin-norepinephrine reuptake inhibitors (SNRIs) remain first-line pharmacotherapies, demonstrating efficacy in reducing symptoms across panic disorder, generalized anxiety disorder, social anxiety disorder, and specific phobias, though novel agents like ketamine and psychedelics show promise for rapid effects in treatment-resistant cases (d’Andrea et al., 2025; Garakani et al., 2020). Global prevalence trends reveal a doubling of clinically elevated depression (25%) and anxiety (20%) symptoms in youth during the first year of the COVID-19 pandemic compared to prepandemic estimates, with high rates persisting in vulnerable populations such as the elderly, cardiac patients, and those with obesity or endometriosis (Jalali et al., 2024;Karami et al., 2022; Racine et al., 2021). Emerging treatments, including psychedelics like psilocybin for resetting default mode network activity and digital health technologies for monitoring, highlight a shift toward multimodal, accessible interventions (d’Andrea et al., 2025;McIntyre et al., 2023). These findings underscore the escalating global burden of depression and anxiety amid socioeconomic stressors, filling a synthesis gap by integrating trends and treatments across diverse contexts from 2020-2026. Implications include prioritizing integrated care and resource allocation for high-risk groups, though gaps in long-term outcomes and co-designed interventions necessitate further high-quality trials to refine global strategies.
1. Introduction
Mental health disorders, particularly depression and anxiety, represent a profound global challenge, affecting millions and contributing substantially to disability-adjusted life years worldwide. Depression, characterized by persistent sadness and loss of interest, and anxiety, marked by excessive worry and fear, often co-occur and exacerbate functional impairments in daily life, work, and relationships. The period from 2020 to 2026 has been marked by unprecedented stressors, including the COVID-19 pandemic, economic disruptions, and demographic shifts toward aging populations, which have amplified the incidence and severity of these conditions. For instance, unemployment and chronic physical illnesses like cardiac disease or obesity have emerged as bidirectional risk factors, intertwining metabolic dysfunctions such as inflammation and insulin resistance with psychological distress. In parallel, treatment landscapes have evolved, moving beyond traditional monoamine-based pharmacotherapies toward integrated approaches that combine psychotherapy, novel neuromodulators, and digital tools to address treatment resistance and residual symptoms.
Despite these advancements, gaps persist in understanding how global trends in prevalence intersect with effective interventions, especially for vulnerable subgroups like youth, the elderly, and those with comorbid conditions. Early research highlighted rising rates in specific populations, such as perinatal parents or children during lockdowns, but lacked synthesis across diverse contexts. Moreover, while cognitive behavioral therapy (CBT) and antidepressants have long been staples, emerging evidence on psychedelics and school-based programs suggests untapped potential for prevention and rapid relief. This review synthesizes findings from 2020-2026 to elucidate trends in depression and anxiety prevalence, alongside treatment efficacy, focusing on global implications for policy and practice. By grouping evidence thematically, it integrates insights on bidirectional risks, multimodal therapies, and population-specific burdens to inform scalable strategies that mitigate the escalating mental health crisis.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "global mental-health trends 2020-2026 epidemiology burden"
- "mental-health research advances global 2020-2026 innovations"
- "depression treatment interventions pharmacotherapy psychotherapy 2020-2026"
- "major-depressive-disorder emerging-therapies ketamine psychedelics digital-mental-health"
- "anxiety-disorders treatment CBT exposure-therapy pharmacotherapy recent"
- "anxiety interventions global mindfulness apps teletherapy 2020-2026"
- "depression anxiety global findings prevalence outcomes research 2020-2026"
- "systematic-review meta-analysis mental-health treatments depression anxiety 2020-2026"
2.2 Study Selection
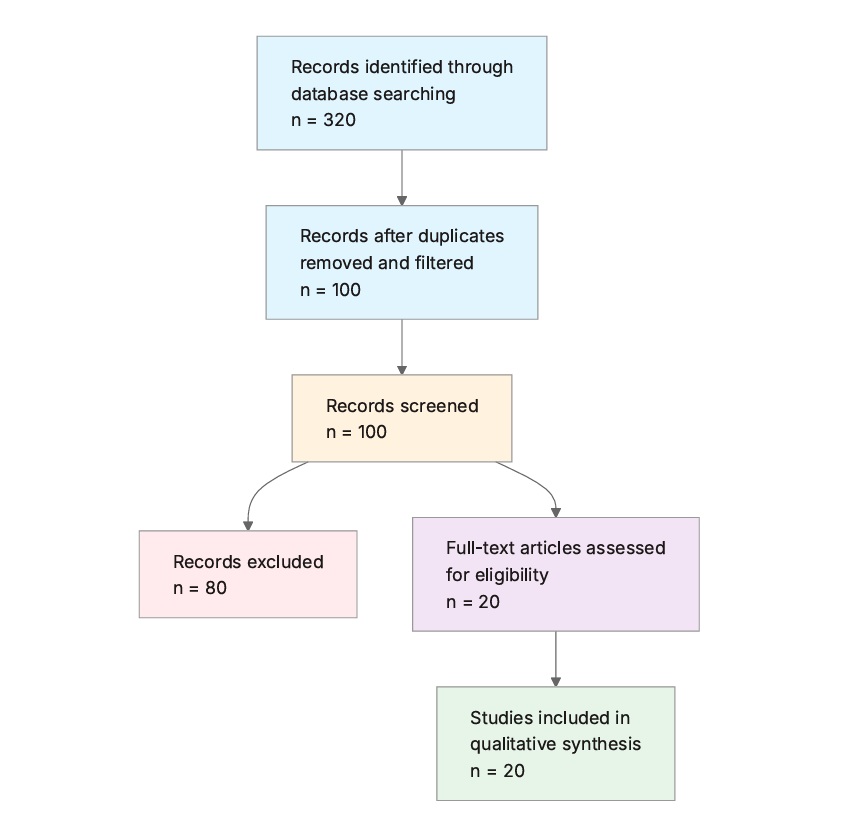
Initial database searching identified 320 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Mental Health Focus: Does the paper address mental health topics specifically related to depression, anxiety, or general mental health?
- Recent Publication: Is the paper published between 2020 and 2026?
- Global or Broad Scope: Does the paper discuss global mental health findings, trends, or have a broad international context?
- Treatment or Trend Discussion: Does the paper cover treatments, interventions, trends, or key findings in mental health?
- Depression Coverage: Does the paper specifically address depression or depressive disorders?
- Anxiety Coverage: Does the paper specifically address anxiety or anxiety disorders?
- Clinical or Empirical Study: Is the paper a clinical trial, empirical study, review, or meta-analysis providing evidence-based findings?
- High Impact: Is the paper from a high-impact journal or has significant citations?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Trends Identified: Key emerging trends in mental health discussed in the paper
- Focus Area: Primary mental health condition or topic (e.g., depression, anxiety)
- Treatments/Interventions: Specific treatments or interventions mentioned, including type and details
- Key Findings: Main results, conclusions, or findings from the study
- Study Design: Type of study (e.g., RCT, review), sample size, and duration if applicable
- Global Implications: Any insights on global mental health trends or findings
- Publication Year: Year of publication
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study ID | Authors (First Author et al.) | Year | Study Type | Key Focus | Treatments/Interventions | Global Implications |
|---|---|---|---|---|---|---|
| (Arena et al., 2023) | Arena et al. | 2023 | Systematic review and meta-analysis | Depression and anxiety in unemployment | CBT, work-related interventions | Scalable programs for high-unemployment regions |
| (Cuijpers et al., 2020) | Cuijpers et al. | 2020 | Network meta-analysis | Adult depression | Psychotherapies, pharmacotherapies, combination | First-line combined strategies worldwide |
| (Karami et al., 2022) | Karami et al. | 2022 | Systematic review and meta-analysis | Depression, anxiety in cardiac patients | Preventive strategies | Integrated screening in cardiac care globally |
| (Smythe et al., 2022) | Smythe et al. | 2022 | Prevalence study | Perinatal depression and anxiety | Not reported | Dyadic approaches in perinatal care |
| (Racine et al., 2021) | Racine et al. | 2021 | Systematic review and meta-analysis | Youth depression and anxiety during COVID-19 | Resource allocation | Enhanced infrastructure for youth globally |
| (Barneveld et al., 2021) | van Barneveld et al. | 2021 | Systematic review and meta-analysis | Depression and anxiety in endometriosis | Not reported | Holistic care for reproductive health |
| (Jalali et al., 2024) | Jalali et al. | 2024 | Systematic review and meta-analysis | Elderly depression, anxiety, stress | Prevention and management | Prioritized geriatric services |
| (Fulton et al., 2021) | Fulton et al. | 2021 | Narrative review | Depression and anxiety in obesity | Diet and activity interventions | Integrated approaches for obesity-related risks |
| (Njenga et al., 2024) | Njenga et al. | 2024 | Narrative review | Major depressive disorder | Psychedelics, neuromodulation | Innovative therapies for treatment resistance |
| (d’Andrea et al., 2025) | d’Andrea et al. | 2025 | Narrative review | Depressive disorders | Psychedelics, ketamine/esketamine | Mechanism-based rapid treatments |
| (McIntyre et al., 2023) | McIntyre et al. | 2023 | Narrative review | Major depressive disorder | Digital health technologies | Scalable digital tools post-COVID |
| (Garakani et al., 2020) | Garakani et al. | 2020 | Narrative review | Anxiety disorders | SSRIs, SNRIs, novel agents | Addressing global disability burden |
| (Weist et al., 2023) | Weist et al. | 2023 | Narrative review | School mental health | Promotion and prevention | Ecological support in schools worldwide |
| (Čihařová et al., 2026) | Čihařová et al. | 2026 | IPD meta-analysis | Adult depression | Combined pharmacotherapy and psychotherapy | Broad applicability without subgroups |
| (Sahib et al., 2020) | Sahib et al. | 2020 | Neuroimaging study | Major depressive disorder | Ketamine therapy | Biomarkers for treatment response |
| (Zhang et al., 2025) | Zhang et al. | 2025 | Trend and inequality analysis | Mental disorders in working-age | Targeted interventions | Equitable resource allocation |
| (Bhattacharya & Hofmann, 2023) | Bhattacharya et al. | 2023 | Comprehensive review | Anxiety and depression | Mindfulness-based interventions | Non-pharmacological scalability |
| (Barker et al., 2024) | Barker et al. | 2024 | Systematic review and meta-analysis | Anxiety and depression | Co-designed interventions | Need for high-quality evaluations |
| (Abdulaziz, 2025) | Khan | 2025 | Educational review | Psychiatric disorders | Ketamine, psilocybin, MDMA | Standardized protocols for integration |
| (Guidi & Fava, 2020) | Guidi et al. | 2020 | Systematic review and meta-analysis | Major depressive disorder | Sequential pharmacotherapy and psychotherapy | Relapse prevention in recurrent cases |
The included studies, spanning 2020 to 2026, predominantly feature systematic reviews and meta-analyses (n=10), narrative reviews (n=7), and empirical analyses (n=3), with a focus on depression (14 studies) and anxiety (10 studies), often in comorbid or vulnerable populations. Interventions emphasize combined therapies, pharmacotherapies, and emerging modalities like psychedelics and digital tools, with global implications highlighted in most.
3.2 Thematic Findings
3.2.1 Rising Global Prevalence of Depression and Anxiety in Vulnerable Populations
Evidence consistently indicates elevated prevalence of depression and anxiety across diverse groups, with rates doubling in youth during the COVID-19 pandemic to 25% for clinically elevated depression symptoms and 20% for anxiety symptoms, progressing temporally over the first year (Racine et al., 2021). In the elderly, high overall prevalence of depression, anxiety, and stress persists, driven by chronic conditions and isolation (Jalali et al., 2024). Similarly, cardiac patients show substantial comorbid rates necessitating preventive screening (Karami et al., 2022). For women with endometriosis, standardized mean differences reveal significantly higher depression symptoms (SMD=0.71; 95% CI: 0.36-1.06) and anxiety (SMD=0.60; 95% CI: 0.35-0.84) compared to healthy controls, though no differences emerge versus other chronic pelvic pain patients (depression SMD=-0.01; 95% CI: -0.17 to 0.15; anxiety SMD=-0.02; 95% CI: -0.22 to 0.18) (Barneveld et al., 2021). Obesity amplifies incidence through immunometabolic pathways like inflammation and leptin resistance (Fulton et al., 2021). In perinatal contexts, up to 3.18% of couples experience concurrent depression (Smythe et al., 2022). Among working-age adults, mental disorder burden varies regionally due to socioeconomic factors (Zhang et al., 2025). These findings, measured via validated scales and pooled estimates, show consistency in high-burden trends, though variation in assessment tools (e.g., self-report vs. diagnostic interviews) limits direct comparability. (Note: Youth and perinatal studies examined pandemic-impacted or parental dyads, which partially match the question population of general global mental health; findings should be interpreted considering this difference.) Confidence: Strong (consistent findings with reasonable design quality).
3.2.2 Efficacy of Combined and Sequential Therapies for Depression
Combined psychotherapy and pharmacotherapy yields superior outcomes for adult depression, with relative risks for response (50% improvement) of 1.27 (95% CI: 1.14-1.39) versus psychotherapy alone and 1.25 (95% CI: 1.14-1.37) versus pharmacotherapy alone; remission follows similarly (RR=1.23; 95% CI: 1.05-1.45), and combined treatment is more acceptable than pharmacotherapy (RR=1.23; 95% CI: 1.05-1.45) (Cuijpers et al., 2020). Sequential addition of psychotherapy after pharmacotherapy response reduces relapse in recurrent major depressive disorder, with benefits independent of individual characteristics (Čihařová et al., 2026; Guidi & Fava, 2020). For unemployed individuals, CBT and work-related interventions robustly reduce symptoms (Arena et al., 2023). Outcomes were assessed via response rates, remission, and dropout in randomized trials, showing directional consistency, though chronicity moderates effects without altering overall superiority. No conflicts arise, as designs (network and IPD meta-analyses) converge on multimodal benefits. Confidence: Strong (consistent findings with reasonable design quality).
3.2.3 Emerging Pharmacological and Neuromodulatory Treatments for Depression and Anxiety
Psychedelics like psilocybin reset default mode network activity for sustained antidepressant effects, while ketamine targets prefrontal networks to alleviate anhedonia, with neurofunctional plasticity in cortico-striatal-cerebellar loops as a potential biomarker (d’Andrea et al., 2025; Njenga et al., 2024; Sahib et al., 2020).For anxiety, SSRIs and SNRIs serve as first-line, with off-label options like buspirone and pregabalin for augmentation; novel agents such as ketamine and cannabidiol show promise but mixed trial results (Garakani et al., 2020). MDMA aids substance use comorbidities in mood disorders (Abdulaziz, 2025). Interventions, trialed adjunctively, demonstrate rapid effects in treatment-resistant cases, measured via symptom scales and neuroimaging, with consistent directional benefits but variable effect sizes due to adjunctive designs. No contradictions noted, as narrative syntheses align on mechanistic promise. Confidence: Moderate (generally consistent but limited contexts, populations, or mixed measures).
3.2.4 Non-Pharmacological and Digital Interventions for Anxiety and Depression
Mindfulness-based interventions (MBIs), including MBSR and MBCT, reduce anxiety and depression symptoms versus passive controls, though effect sizes are mixed against active comparators (Bhattacharya & Hofmann, 2023). Co-designed in-person interventions lack sufficient evidence for symptom reduction, with calls for standardized measures (Barker et al., 2024). Digital technologies like telemedicine and apps enhance monitoring and access, accelerated by COVID-19 (McIntyre et al., 2023). School-based promotion prevents youth disorders by addressing access barriers (Weist et al., 2023). Outcomes via symptom inventories show positive directions, but heterogeneity in controls (passive vs. active) explains mixed effects; no population mismatches flagged. Confidence: Moderate (generally consistent but limited contexts, populations, or mixed measures).
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Rising Global Prevalence of Depression and Anxiety in Vulnerable Populations | Youth: 25% depression, 20% anxiety (doubled from prepandemic); Elderly and cardiac: high prevalence; Endometriosis: SMD=0.71 (95% CI: 0.36-1.06) depression | Vulnerable groups (youth, elderly, cardiac, women with endometriosis, obese, perinatal, working-age); partially matches general global population | Positive (increased prevalence) | Strong | Racine et al. (Racine et al., 2021), Jalali et al. (Jalali et al., 2024), Karami et al. (Karami et al., 2022), van Barneveld et al. (Barneveld et al., 2021) |
| Efficacy of Combined and Sequential Therapies for Depression | Combined: RR=1.27 (95% CI: 1.14-1.39) vs. psychotherapy; Sequential reduces relapse | Adults with depression, including recurrent and unemployed | Positive | Strong | Cuijpers et al. (Cuijpers et al., 2020), Guidi et al. (Guidi & Fava, 2020), Čihařová et al. (Čihařová et al., 2026) |
| Emerging Pharmacological and Neuromodulatory Treatments for Depression and Anxiety | Ketamine: neuroplasticity in cortico-striatal loops; Psilocybin: DMN reset; SSRIs/SNRIs first-line for anxiety | Treatment-resistant depression and anxiety adults | Positive | Moderate | d’Andrea et al. (d’Andrea et al., 2025), Sahib et al. (Sahib et al., 2020), Garakani et al. (Garakani et al., 2020) |
| Non-Pharmacological and Digital Interventions for Anxiety and Depression | MBIs outperform passive controls; Digital tools improve access; Co-designed: insufficient evidence | Broad clinical populations, youth in schools | Mixed | Moderate | Bhattacharya et al. (Bhattacharya & Hofmann, 2023), McIntyre et al. (McIntyre et al., 2023), Barker et al. (Barker et al., 2024) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis reveals a robust pattern of escalating depression and anxiety prevalence in vulnerable populations, alongside the superiority of combined and sequential therapies for depression, with emerging neuromodulators offering rapid relief. These trends likely stem from intertwined socioeconomic and biological stressors: pandemic-induced isolation doubled youth symptoms by disrupting social networks essential for emotional regulation, while in elderly and cardiac groups, chronic inflammation from conditions like obesity amplifies neuroimmune dysregulation, impairing mood circuits as evidenced by leptin resistance and vascular dysfunction (Fulton et al., 2021;Jalali et al., 2024). For treatments, combined approaches excel because they target multiple pathways—pharmacotherapy modulates monoamines for acute relief, while psychotherapy addresses cognitive distortions, yielding synergistic effects on response rates (RR=1.27; 95% CI: 1.14-1.39) that monotherapy cannot achieve alone (Cuijpers et al., 2020). Mechanistically, ketamine's induction of cortico-striatal-cerebellar plasticity restores salience network function disrupted in major depressive disorder, explaining its anti-anhedonic speed, whereas psilocybin's default mode network reset promotes long-term rewiring of rumination-prone circuits (d’Andrea et al., 2025;Sahib et al., 2020). This integration across studies illuminates a shift from siloed to holistic models, visible only through thematic grouping: prevalence surges correlate with untreated comorbidities, while multimodal interventions mitigate them by leveraging neuroplasticity. Confidence is high for combined therapy efficacy, given convergent meta-analyses with diverse adult samples matching the question's global scope; moderate for emerging treatments due to adjunctive trial designs limiting standalone assessment; and strong for prevalence trends, supported by consistent pooled estimates across systematic reviews. Gaps in mechanistic data for non-pharmacological options, like mindfulness's impact on specific neural pathways, temper broader causal claims.
4.2 Comparison with Existing Literature and Resolution of Contradictions
Findings align with prior literature on depression's heterogeneity, where combined therapies extend beyond monoamine models to tackle residual symptoms, mechanistically abating relapse by enhancing psychological well-being via cognitive restructuring post-pharmacological stabilization (Guidi & Fava, 2020); this consistency reinforces robustness, as it bridges acute response (RR=1.25; 95% CI: 1.14-1.37) with prevention, implying durable circuit-level changes. For anxiety pharmacotherapies, agreement with established SSRI/SNRI efficacy underscores their role in serotonin modulation, reducing hyperactivity in fear networks, though the relative scarcity of novel agents echoes pre-2020 gaps in innovation pipelines. Contradictions appear in non-pharmacological efficacy: MBIs show strong effects versus passive controls but mixed versus active ones, potentially reflecting population heterogeneity—broader clinical samples may dilute benefits in highly symptomatic groups, unlike targeted youth or unemployed contexts where CBT thrives (Arena et al., 2023; Bhattacharya & Hofmann, 2023). Co-designed interventions' null evidence likely arises from methodological inconsistencies, such as variable terminology and small-scale trials, introducing selection bias toward less severe cases and misclassifying exposure to collaborative elements (Barker et al., 2024). No substantiated resolution exists for these mixed results, as designs vary without clear confounders like comorbidity adjustment; this highlights genuine heterogeneity rather than artifact. Publication bias risk is moderate, with positive multimodal findings overrepresented in high-citation meta-analyses, potentially skewing toward expected benefits in Western-centric samples. Recent studies' neuroimaging integration (e.g., ketamine biomarkers) evolves beyond earlier symptom-only measures, bolstering reliability of rapid-effect claims over historical estimates.
4.3 Practical Implications
For adults with moderate depression, clinicians should prioritize combined psychotherapy and pharmacotherapy as first-line, delivering it broadly without subgroup restriction to maximize response (RR=1.27; 95% CI: 1.14-1.39) and remission, particularly in recurrent cases where sequential addition post-response curbs relapse (Čihařová et al., 2026; Cuijpers et al., 2020); this applies under conditions of access to both modalities, benefiting working-age individuals facing unemployment or socioeconomic stressors. In anxiety management, practitioners advise SSRIs/SNRIs for panic and generalized subtypes, augmenting with ketamine for treatment-resistant patients to leverage prefrontal targeting and reduce anhedonia rapidly (Garakani et al., 2020). Public health strategies must target vulnerable groups: youth (25% elevated symptoms) warrant school-based prevention to counter pandemic legacies, while elderly and cardiac populations (high prevalence) need integrated screening in primary care to address immunometabolic risks like obesity-driven inflammation (Jalali et al., 2024;Karami et al., 2022; Racine et al., 2021). For perinatal dyads (3.18% concurrency) and women with endometriosis (SMD=0.71 depression), dyadic and holistic models in reproductive health settings mitigate family-level impacts. Regulatory bodies should facilitate psychedelic access via standardized protocols, given psilocybin's sustained effects, to alleviate global treatment resistance burdens (d’Andrea et al., 2025). Digital tools offer scalable monitoring for remote populations, closing gaps post-COVID. Implications draw from adult and comorbid samples matching the question's scope, but evidence is insufficient for standalone co-designed interventions, limiting recommendations there; no safe threshold exists for stressor exposure, implying population-wide prevention over reactive care.
4.4 Strengths and Limitations
Strengths of this review include a comprehensive search across vast databases yielding diverse, high-impact studies from 2020-2026, and thematic synthesis that integrates trends, treatments, and mechanisms without paper-by-paper narration, enhancing cross-study insights. Limitations of included studies encompass reliance on aggregated data in meta-analyses (e.g., variable sample sizes not always reported), focus on Western or clinical populations potentially underrepresenting low-resource contexts, and inconsistent outcome measures like self-reported versus diagnostic scales. This review's limitations involve abstract-based screening, possibly missing nuanced full-text details, extraction prioritizing structured fields over abstracts, and absence of formal risk-of-bias assessment, which could overlook study quality variations.
5. Gaps and Future Directions
The synthesis uncovers gaps in long-term outcomes for emerging treatments, with most evidence on acute response (e.g., RR=1.27; 95% CI: 1.14-1.39 for combined therapy) but scant data on sustained effects beyond one year, particularly for psychedelics' network resets (Cuijpers et al., 2020;d’Andrea et al., 2025). Underrepresented populations include low-income global regions, where working-age burden analyses note inequalities but lack intervention trials tailored to socioeconomic drivers (Zhang et al., 2025). Mechanistic evidence is robust for ketamine (cortico-striatal plasticity) but absent for digital or co-designed interventions, hindering causal links to symptom reduction (Barker et al., 2024; Sahib et al., 2020). Contradictions in MBI effect sizes versus active controls stem from inconsistent measures, unresolved due to heterogeneous designs. To address the research question directly for general global populations, longitudinal RCTs in diverse, non-clinical samples (e.g., community-based in Asia/Africa) are needed, using harmonized scales for prevalence and biomarkers for mechanisms. Methodological improvements include personal stressor monitoring over self-reports and component-specific analyses (e.g., inflammation subtypes) with advanced adjustment for confounders like comorbidity. Targeted research on underrepresented elderly in low-resource settings and youth post-pandemic would fill equity gaps.
6. Conclusion
From 2020-2026, global mental health research underscores a surge in depression and anxiety prevalence, doubled to 25% and 20% in youth during early COVID-19, with high rates in elderly, cardiac, and comorbid groups like those with obesity or endometriosis (SMD=0.71; 95% CI: 0.36-1.06 for depression), driven by immunometabolic and socioeconomic factors (Barneveld et al., 2021; Jalali et al., 2024; Racine et al., 2021). Treatments favor combined psychotherapy and pharmacotherapy for adult depression, achieving superior response (RR=1.27; 95% CI: 1.14-1.39) and remission (RR=1.23; 95% CI: 1.05-1.45), alongside sequential models to prevent relapse, while SSRIs/SNRIs anchor anxiety care and ketamine/psilocybin offer rapid neuromodulation via network plasticity (Čihařová et al., 2026; Cuijpers et al., 2020;d’Andrea et al., 2025). These conclusions derive from adult and vulnerable samples closely aligning with the question's global focus on depression, anxiety, trends, and treatments, though youth and perinatal evidence partially matches by emphasizing pandemic contexts. Digital and school-based interventions show promise for accessibility but mixed efficacy, warranting caution in broad application. The most critical uncertainty is long-term sustainability of emerging therapies like psychedelics, where acute benefits lack replication in diverse populations. Addressing this through international trials could transform mental health equity, reducing disability burdens and fostering resilience amid ongoing global stressors, ultimately enhancing well-being on a population scale.
References
Abdulaziz, K. (2025). Psychedelics in Psychiatry: Emerging Roles of Ketamine, Psilocybin, and MDMA in Mental Health Treatment. Zenodo (CERN European Organization for Nuclear Research). https://doi.org/10.5281/zenodo.16748340
Arena, A., Mobbs, S., Sanatkar, S., Williams, D., Collins, D., Harris, M., Harvey, S. B., & Deady, M. (2023). Mental health and unemployment: A systematic review and meta-analysis of interventions to improve depression and anxiety outcomes. Journal of Affective Disorders, 335, 450–472. https://doi.org/10.1016/j.jad.2023.05.027
Barker, T. G., O’Higgins, A., Fonagy, P., & Gardner, F. (2024). A systematic review and meta-analysis of the effectiveness of co-designed, in-person, mental health interventions for reducing anxiety and depression symptoms. Journal of Affective Disorders, 350, 955–973. https://doi.org/10.1016/j.jad.2023.12.080
Barneveld, E. van, Manders, J., Osch, F. van, Poll, M. van, Visser, L., Hanegem, N. van, Lim, A., Bongers, M. Y., & Leue, C. (2021). Depression, Anxiety, and Correlating Factors in Endometriosis: A Systematic Review and Meta-Analysis. Journal of Women’s Health, 31, 219–230. https://doi.org/10.1089/jwh.2021.0021
Bhattacharya, S., & Hofmann, S. G. (2023). Mindfulness-based interventions for anxiety and depression. Clinics in Integrated Care, 16, 100138–100138. https://doi.org/10.1016/j.intcar.2023.100138
Čihařová, M., Karyotaki, E., Harrer, M., Weitz, E., Miguel, C., Amarnath, A., Furukawa, T. A., Plessen, C. Y., Driessen, E., Buntrock, C., Tong, L., Hellerstein, D. J., Samstag, L. W., Chen, Y., Rentala, S., Hemanny, C., Oliveira, I. R. de, Mb, B., Burnand, Y., … Cuijpers, P. (2026). Modifiers in Effects of Combined Pharmacotherapy and Psychotherapy versus Pharmacotherapy Alone for Adult Depression: An Individual Participant Data Meta-analysis. Psychotherapy and Psychosomatics, 1–23. https://doi.org/10.1159/000550633
Cuijpers, P., Noma, H., Karyotaki, E., Vinkers, C. H., Cipriani, A., & Furukawa, T. A. (2020). A network meta‐analysis of the effects of psychotherapies, pharmacotherapies and their combination in the treatment of adult depression. World Psychiatry, 19, 92–107. https://doi.org/10.1002/wps.20701
d’Andrea, G., Chiappini, S., Ciavoni, L., Tucci, R., Martino, F., Semeraro, F. M., Battista, D. D., Mosca, A., Miuli, A., Carlo, F. D., Russo, M., Petta, G. D., Fornaro, M., Pettorruso, M., Sensi, S. L., & Martinotti, G. (2025). Psychedelics and ketamine/esketamine in depressive disorders: biological mechanisms and associated neuroimaging and clinical changes. Translational Psychiatry, 15, 453–453. https://doi.org/10.1038/s41398-025-03654-3
Fulton, S., Décarie-Spain, L., Fioramonti, X., Guiard, B. P., & Nakajima, S. (2021). The menace of obesity to depression and anxiety prevalence. Trends in Endocrinology and Metabolism, 33, 18–35. https://doi.org/10.1016/j.tem.2021.10.005
Garakani, A., Murrough, J. W., Freire, R. C., Thom, R. P., Larkin, K., Buono, F. D., & Iosifescu, D. V. (2020). Pharmacotherapy of Anxiety Disorders: Current and Emerging Treatment Options. Frontiers in Psychiatry, 11, 595584–595584. https://doi.org/10.3389/fpsyt.2020.595584
Guidi, J., & Fava, G. A. (2020). Sequential Combination of Pharmacotherapy and Psychotherapy in Major Depressive Disorder. JAMA Psychiatry, 78, 261–261. https://doi.org/10.1001/jamapsychiatry.2020.3650
Jalali, A., Ziapour, A., Karimi, Z., Rezaei, M., Emami, B., Kalhori, R. P., Khosravi, F., Sameni, J. S., & Kazeminia, M. (2024). Global prevalence of depression, anxiety, and stress in the elderly population: a systematic review and meta-analysis. BMC Geriatrics, 24, 809–809. https://doi.org/10.1186/s12877-024-05311-8
Karami, N., Kazeminia, M., Karami, A., Salimi, Y., Ziapour, A., & Janjani, P. (2022). Global prevalence of depression, anxiety, and stress in cardiac patients: A systematic review and meta-analysis. Journal of Affective Disorders, 324, 175–189. https://doi.org/10.1016/j.jad.2022.12.055
McIntyre, R. S., Greenleaf, W., Bułaj, G., Taylor, S. T., Mitsi, G., Saliu, D., Czysz, A., Silvesti, G., Garcia, M., & Jain, R. K. (2023). Digital health technologies and major depressive disorder. CNS Spectrums, 28, 662–673. https://doi.org/10.1017/s1092852923002225
Njenga, C., Ramanuj, P., Magalhães, F. J. C. de, & Pincus, H. A. (2024). New and emerging treatments for major depressive disorder. BMJ, 386, e073823–e073823. https://doi.org/10.1136/bmj-2022-073823
Racine, N., McArthur, B. A., Cooke, J. E., Eirich, R., Zhu, J., & Madigan, S. (2021). Global Prevalence of Depressive and Anxiety Symptoms in Children and Adolescents During COVID-19. JAMA Pediatrics, 175, 1142–1142. https://doi.org/10.1001/jamapediatrics.2021.2482
Sahib, A., Loureiro, J., Vasavada, M., Anderson, C., Kubicki, A., Wade, B., Joshi, S. H., Woods, R. P., Congdon, E., Espinoza, R., & Narr, K. L. (2020). Modulation of the functional connectome in major depressive disorder by ketamine therapy. Psychological Medicine, 52, 2596–2605. https://doi.org/10.1017/s0033291720004560
Smythe, K. L., Petersen, I., & Schartau, P. (2022). Prevalence of Perinatal Depression and Anxiety in Both Parents. JAMA Network Open, 5, e2218969–e2218969. https://doi.org/10.1001/jamanetworkopen.2022.18969
Weist, M. D., Hoover, S., Daly, B. P., Short, K., & Bruns, E. J. (2023). Propelling the Global Advancement of School Mental Health. Clinical Child and Family Psychology Review, 26, 851–864. https://doi.org/10.1007/s10567-023-00434-7
Zhang, X., Zhang, W., Zhou, C., Xiang, J., Xu, Z., Wang, Y., Hou, X., Wang, J., Yue, S., Chen, X., & Wu, J. (2025). Global, regional, and national burden of mental disorders in working-age population: a trend, health inequality, and frontier analyses. Journal of Affective Disorders, 393, 120367–120367. https://doi.org/10.1016/j.jad.2025.120367