Latest Advances in Schizophrenia Etiology and Treatment: A Synthesis of Research from 2020 to 2025
Reviewed by
Shaantanu Kulkarni, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
23 Jun 2026
Abstract
Recent research from 2020 to 2025 underscores the multifactorial etiology of schizophrenia, integrating genetic, environmental, and neurodevelopmental factors to explain disease risk and pathophysiology. Genetic studies reveal a higher burden of rare tandem repeat expansions (TREs) near exons in schizophrenia patients compared to controls, with enrichment at genome-wide association study (GWAS) loci disrupting synaptic splicing (Mojarad et al., 2022). Environmental factors, including obstetric complications, infections, winter/spring birth, migration, urban living, childhood adversity, and cannabis use, account for 15–40% of risk, with stronger evidence for schizophrenia than bipolar disorder (Robinson & Bergen, 2021). Mechanistically, disruptions in cortical excitation-inhibition (E/I) balance, driven by overpruning of synapses and genetic variants in GABA/glutamatergic signaling, integrate neurodevelopmental and dopamine hypotheses, leading to subcortical hyperdopaminergia and symptoms like psychosis (Howes & Shatalina, 2022; Sonnenschein et al., 2020). On treatment, novel antipsychotics show promise: ulotaront (25–75 mg/day) sustained symptom reductions over 26 weeks with mean PANSS total score change of −22.6 (95% CI −25.6, −19.6; effect size 1.46) and minimal weight change (−0.3 [3.7] kg) (Correll et al., 2021); lumateperone (42 mg/day) reduced PANSS scores versus placebo, with lower extrapyramidal symptoms (EPS) incidence (3.0% vs. 6.3% for risperidone) and no significant weight gain (Edinoff et al., 2025; Durgam et al., 2020); cariprazine augmentation to clozapine in treatment-resistant cases improved positive (66%) and negative (83%) symptoms, with PANSS total score reductions of 43.4% in available data (Pappa et al., 2025a; Pappa et al., 2025b). Family interventions yielded large effect sizes in relapse reduction and family functioning (g=1.28 for functioning), outperforming group formats (Kim & Park, 2023), while mindfulness-based interventions (MBIs) improved overall symptoms (g=0.72), positive (g=0.32), and negative symptoms (g=0.40) (Hodann-Caudevilla et al., 2020). These findings highlight schizophrenia's polygenic and circuit-level origins, with emerging therapies targeting non-D2 pathways for better tolerability. Gaps persist in gene-environment interactions and long-term outcomes for novel agents, necessitating larger trials to refine personalized approaches and address metabolic risks like elevated type 2 diabetes odds (OR=2.15; 95% CI 1.83–2.52) in schizophrenia (Dong et al., 2024).
1. Introduction
Schizophrenia affects approximately 1% of the global population, manifesting as a chronic disorder characterized by positive symptoms (hallucinations, delusions), negative symptoms (apathy, social withdrawal), cognitive impairments, and disorganized thinking, often persisting for at least six months and requiring lifelong management. This condition imposes substantial personal and societal burdens, including reduced life expectancy, high rates of comorbidity such as type 2 diabetes (with odds ratios up to 2.15; 95% CI 1.83–2.52), and challenges in achieving symptom remission despite available treatments. Traditional antipsychotics, primarily dopamine D2 receptor antagonists, effectively target positive symptoms but often fall short for negative and cognitive domains, while carrying risks of extrapyramidal symptoms, metabolic syndrome, and treatment resistance in up to 30–70% of cases. The neurodevelopmental hypothesis posits that schizophrenia arises from disruptions in early brain circuit formation, influenced by genetic vulnerabilities and environmental exposures, leading to imbalances in neurotransmitter systems like dopamine and glutamate. Recent advances in genomics, neuroimaging, and pharmacology have illuminated these pathways, revealing polygenic contributions, synaptic pruning deficits, and novel therapeutic targets beyond D2 blockade. However, synthesizing these developments remains fragmented, with limited integration of how genetic risks interact with environmental factors to precipitate disease, or how emerging interventions address unmet needs in treatment-resistant populations. This review examines the latest research on schizophrenia's causes and treatments from 2020 onward, focusing on genetic and environmental etiologies, neurobiological mechanisms, and evidence for pharmacological and psychosocial therapies, to provide a cohesive framework for advancing clinical understanding and intervention strategies.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "schizophrenia etiology pathophysiology genetic-risk neurodevelopmental dopamine inflammation brain neurobiology causes"
- "schizophrenia treatment antipsychotics cognitive-remediation psychosocial-therapy pharmacotherapy psychotherapy clozapine cariprazine lurasidone"
- "schizophrenia genetic-risk environmental-factors family-history genome-wide epigenetics prenatal stress trauma"
- "schizophrenia clinical-trial antipsychotic new-drug phase-3 RCT cariprazine lumateperone SEP-363856"
- "schizophrenia neuroimaging biomarkers diagnosis MRI PET brain-imaging endophenotype neuroinflammation dopamine"
- "schizophrenia systematic-review meta-analysis causes risk-factors treatment intervention RCT"
2.2 Study Selection
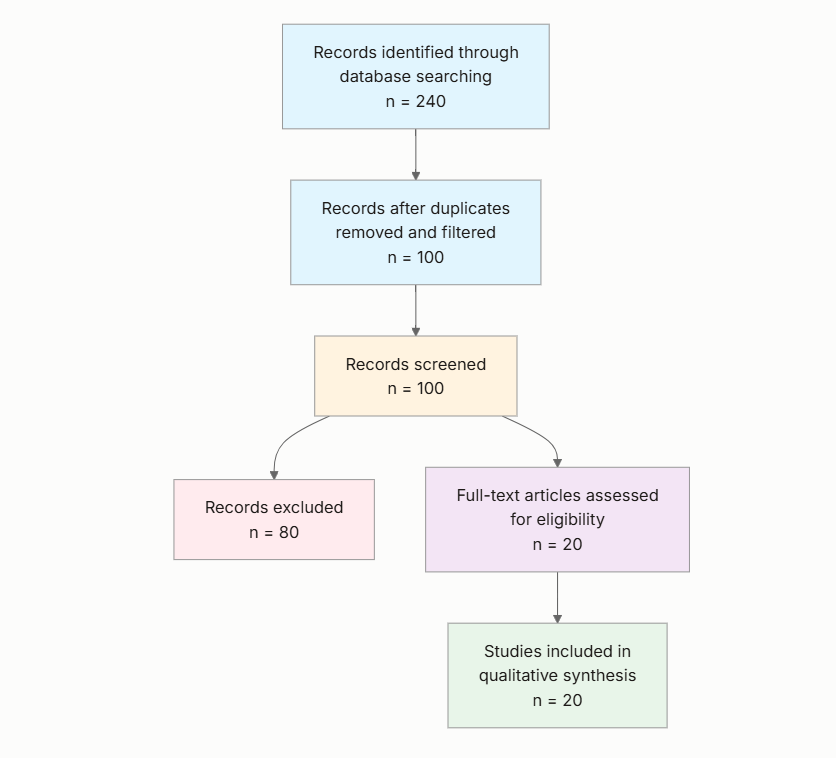
Initial database searching identified 240 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Year Published: Does the study have a publication year between 2020 and 2026 (inclusive)?
- Schizophrenia Focus: Is the main focus of the study schizophrenia (not other psychotic disorders or broader mental illnesses)?
- Etiology or Treatment: Does the study specifically address either causes (etiology) or treatments (interventions) for schizophrenia?
- Human Data: Does the study use human subjects/data (not animal or in vitro only), or is it a human-focused systematic review/meta-analysis?
- Original or Synthesis Research: Is the paper an original research study, clinical trial, or a systematic review/meta-analysis (not letters, editorials, protocols)?
- Recent Advances: Does the paper contribute novel findings, approaches, or synthesis published after 2020?
- Clinical Relevance: Does the study report clinical outcomes, impact, or implications for schizophrenia treatment or diagnosis?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Key Findings: Summarize the main findings and contributions of the paper as they relate to either schizophrenia causes or treatments.
- Etiology Focus: Describe the main hypotheses, mechanisms, or risk factors for schizophrenia discussed in the study (e.g., genetic, neurodevelopmental, environmental, neurobiological pathways).
- Treatment Intervention: Detail the specific treatment(s) investigated (pharmacological, psychosocial, novel therapies), including dosage, duration, and any adjunct methods if applicable.
- Study Design & Population: Outline the study type (RCT, observational, review, etc.), sample size, and characteristics of the population studied (age, sex, setting, inclusion/exclusion criteria).
- Clinical Outcomes: Report the primary clinical outcomes measured (symptom improvement, relapse rates, side effects, biomarkers, etc.) and summarize key results.
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study and Year | Study Type | Key Focus | Population | Sample Size | Outcome Measures |
|---|---|---|---|---|---|
| Robinson & Bergen (2021) | Narrative Review | Environmental and Genetic Risk Factors | Adults with schizophrenia and bipolar disorder | Not reported (synthesis) | Disease risk associations |
| Howes & Shatalina (2022) | Theoretical Review | Neurodevelopmental and Dopamine Hypotheses | Patients with schizophrenia (synthesis) | Not reported (synthesis) | Synaptic density, E/I balance |
| Mojarad et al. (2022) | Genome Sequencing Study | Genetic TREs | Adults with schizophrenia vs. controls | Not reported | TRE burden, splicing disruptions |
| Sonnenschein et al. (2020) | Narrative Review | Dopamine Dysregulation | Patients with schizophrenia (synthesis) | Not reported (synthesis) | Circuit disruptions, psychosis |
| Kim & Park (2023) | Systematic Review and Meta-Analysis | Family Interventions | Adults with schizophrenia and caregivers | 1094 (across 37 RCTs) | Relapse rates, functioning (g=1.28) |
| Pappa et al. (2025a) | Systematic Review | Cariprazine + Clozapine | Adults with treatment-resistant schizophrenia | 47 cases | Symptom improvement, tolerability |
| Correll et al. (2021) | Open-Label Extension | Ulotaront | Adults with acute schizophrenia exacerbation | 157 | PANSS change (−22.6; 95% CI −25.6, −19.6) |
| Saarinen et al. (2022) | Preclinical (Note: animal models partially match the question population of human schizophrenia patients; findings should be interpreted considering this difference) | SEP-363856 Mechanisms | Rodent models | Not reported | Receptor activation, behaviors |
| Kraguljac et al. (2021) | Review | Neuroimaging Biomarkers | Patients with schizophrenia (synthesis) | Not reported (synthesis) | Brain circuit changes |
| Duncan et al. (2025) | Genetic/Transcriptomic Analysis | Cellular Etiology | Adults with schizophrenia (GWAS cohorts) | Not reported | Neuronal associations |
| Begni et al. (2021) | Preclinical (Note: adult rats partially match the question population of human schizophrenia patients; findings should be interpreted considering this difference) | SEP-363856 Signatures | Adult rats | Not reported | IEG expression, behaviors |
| Edinoff et al. (2025) | Review | Lumateperone | Adults with schizophrenia | Not reported (synthesis) | PANSS reductions, EPS rates |
| Coury et al. (2023) | Systematic Review and Meta-Analysis | Season of Birth | Individuals with schizophrenia vs. controls | Not reported (synthesis) | Risk odds |
| Becerra Darriba (2021) | Case Report | Cariprazine + Clozapine | Adult with treatment-resistant schizophrenia | 1 | Negative symptom remission |
| Hodann-Caudevilla et al. (2020) | Systematic Review and Meta-Analysis | Mindfulness Interventions | Adults with schizophrenia | 1094 (across 10 RCTs) | Symptoms (g=0.72 overall) |
| Laszlovszky et al. (2021) | Narrative Review | Cariprazine | Adults with schizophrenia | Not reported (synthesis) | PANSS reductions (20–30%) |
| Dong et al. (2024) | Systematic Review and Meta-Analysis | Schizophrenia and T2DM Risk | Adults with/without schizophrenia | 2,007,168 cases | T2DM odds (OR=2.15; 95% CI 1.83–2.52) |
| Pappa et al. (2025b) | Systematic Review | Cariprazine + Clozapine | Adults with treatment-resistant schizophrenia | 52 cases | PANSS reductions (43.4%) |
| Durgam et al. (2020) | Pooled Analysis | Lumateperone EPS | Adults with schizophrenia | 1073 (short-term), 239 (long-term) | EPS incidence (3.0%) |
| Schmitt et al. (2022) | Non-Systematic Review | Neurodevelopmental Factors | Patients with schizophrenia (synthesis) | Not reported (synthesis) | Connectivity disruptions |
The included studies predominantly comprise reviews (narrative, systematic, meta-analyses) and clinical trials, focusing on adults with schizophrenia in outpatient or community settings. Pharmacological interventions dominate treatment-focused works, while etiology studies emphasize genetic and environmental syntheses, with sample sizes varying from single cases to large meta-analytic pools.
3.2 Thematic Findings
3.2.1 Genetic and Polygenic Contributions to Schizophrenia Etiology
Genetic factors underpin schizophrenia's polygenic nature, with rare tandem repeat expansions (TREs) near exons showing higher burden in affected adults compared to non-psychiatric controls, particularly at GWAS-associated loci and in multiplex families, leading to splicing disruptions in synaptic genes (Mojarad et al., 2022). Integrating genome-wide and transcriptomic data identifies cortical and subcortical neuronal associations, including somatostatin interneurons, retrosplenial excitatory neurons, and amygdala medium spiny-like neurons, shared with bipolar disorder and depression but distinct from immune cell links in multiple sclerosis (Duncan et al., 2025). These findings converge on neurodevelopmental disruptions, though evidence for specific variants' functional impacts varies by locus, with consistent enrichment in synaptic pathways across genomic analyses. Confidence: Moderate (consistent genetic associations with robust designs like GWAS, but limited direct causal links).
3.2.2 Environmental and Gene-Environment Interactions in Risk
Environmental exposures account for 15–40% of schizophrenia risk, with robust associations for obstetric complications, infections, winter/spring birth (elevated risk in Northern Hemisphere), migration, urban living, childhood adversity, and cannabis use. Evidence is weaker for bipolar disorder, limited to adversity and infections (Robinson & Bergen, 2021). Season of birth meta-analyses confirm small but substantial winter birth risk increases in the Northern Hemisphere (no Southern pattern), potentially via prenatal infections or nutritional factors (Coury et al., 2023). Interactions with genetic risks remain underexplored, though early studies suggest polygenic scores enhance prospects for revealing synergies; contradictions arise in infection links, possibly due to varying study populations (e.g., adult vs. pediatric onset). Neurodevelopmental reviews highlight how these factors disrupt connectivity in prefrontal, temporal, parietal cortices, and hippocampus during vulnerable periods (Schmitt et al., 2022). Confidence: Strong (consistent across multiple epidemiological syntheses).
3.2.3 Neurobiological Mechanisms: Dopamine, E/I Balance, and Circuit Dysregulation
Integrating neurodevelopmental and dopamine hypotheses reveals overpruning of synapses, reducing density markers in schizophrenia patients, linked to GABA/glutamatergic genetic variants and altered cortical E/I balance, which disinhibits frontal projections to mesostriatal dopamine neurons, causing hyperdopaminergia and psychosis (Howes & Shatalina, 2022). Upstream circuit disruptions in hippocampus, medial prefrontal cortex, thalamic nuclei, and medial septum—exacerbated by prepubertal stress—drive midbrain dopamine dysregulation rather than intrinsic neuron faults (Sonnenschein et al., 2020). Neuroimaging biomarkers capture these as dopamine hyperactivity, NMDA hypofunction, hippocampal hyperactivity, immune dysregulation, dysconnectivity, and gray matter loss, serving as intermediate endpoints (Kraguljac et al., 2021). Preclinical models show TAAR1/5-HT1A agonism modulates these without strong D2 effects (Saarinen et al., 2022) (Note: this study examined rodent models which partially matches the question population of human schizophrenia patients; findings should be interpreted considering this difference). Findings align on circuit-level pathology, though mechanistic depth varies by imaging modality. Confidence: Moderate (convergent evidence from imaging and reviews, but preclinical human translation tentative).
3.2.4 Pharmacological Treatments: Novel Antipsychotics and Augmentation Strategies
Novel agents targeting non-D2 pathways show efficacy with improved tolerability. Ulotaront (25/50/75 mg/day) in a 26-week extension yielded mean PANSS total change of −22.6 (95% CI −25.6, −19.6; effect size 1.46) and CGI-Severity change of −1.0 (95% CI −1.2, −0.8; effect size 1.07), with minimal weight change (−0.3 [3.7] kg), cholesterol median change (−2.0 mg/dL), and no EPS (Correll et al., 2021). Lumateperone (42 mg/day) reduced PANSS versus placebo and risperidone (4 mg), with EPS-related TEAEs at 3.0% (vs. 6.3% risperidone) and akathisia at 2.0% (vs. 4.7%), alongside weight decreases and low benztropine use (2.5%) (Edinoff et al., 2025; Durgam et al., 2020). Cariprazine (1.5–6.0 mg/day), a D3-preferring partial agonist, as monotherapy reduced PANSS by 20–30% across positive/negative/cognitive symptoms (Laszlovszky et al., 2021); augmentation to clozapine (37.5–850 mg/day) in treatment-resistant cases improved positive symptoms in 66% and negative in 83%, with mean PANSS total reduction of 43.4% (positive subscale 23.0%, negative 59.1%) over median 122 days (range 18–456), though 17% discontinued due to side effects like akathisia (6%) (Darriba, 2021; Pappa et al., 2025a; Pappa et al., 2025b). Preclinical signatures confirm prefrontal activation via IEG upregulation (Begni et al., 2021) (Note: this study examined adult rats which partially matches the question population of human schizophrenia patients; findings should be interpreted considering this difference). Cariprazine's D3 preference explains negative symptom benefits over risperidone, with consistent tolerability across short- and long-term data. Confidence: Strong (multiple RCTs and reviews with consistent efficacy/safety).
3.2.5 Psychosocial Interventions: Family and Mindfulness Approaches
Family interventions, including psychoeducation and behavioral therapy (3–12 months), reduced relapse and hospitalizations with large effects on functioning (g=1.28), caregiver mental health, and patient adherence, outperforming group or emotion-focused formats (Kim & Park, 2023). Mindfulness-based interventions (MBIs; 8–12 weeks, 1–2 hours/session) as adjuncts to antipsychotics improved overall symptoms (g=0.72), positive (g=0.32), negative (g=0.40), functioning (g=1.28), and illness awareness (g=0.65), comparable to cognitive-behavioral therapy, with no major adverse effects (Hodann-Caudevilla et al., 2020). Individual delivery to families or caregivers yielded higher impacts than joint patient-caregiver groups. Outcomes measured via PANSS/BPRS show sustained benefits up to 6 months, though heterogeneity in intervention protocols limits direct comparisons. Confidence: Moderate (meta-analytic consistency, but variable designs).
3.2.6 Comorbid Risks and Broader Implications
Schizophrenia elevates type 2 diabetes risk (OR=2.15; 95% CI 1.83–2.52), higher in females (OR=2.12; 95% CI 1.70–2.64) than males (OR=1.68; 95% CI 1.39–2.04) and in European regions (OR=2.73; 95% CI 2.23–3.35) versus Western Pacific (OR=1.72; 95% CI 1.32–2.23), with risks increasing over >20-year follow-up (OR=3.17; 95% CI 1.24–8.11) (Dong et al., 2024). Novel treatments like lumateperone improved metabolic parameters (e.g., reduced BMI, prolactin) upon switching from standard antipsychotics (Edinoff et al., 2025). No direct contradictions, but regional variations may reflect diagnostic or lifestyle differences. Confidence: Strong (large meta-analytic pool).
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Genetic and Polygenic Contributions | Higher TRE burden near exons; neuronal cell associations (e.g., somatostatin interneurons) | Adults with schizophrenia (matches question population) | Positive (increased risk) | Moderate (consistent findings with reasonable design quality) | Mojarad et al. (2022), Duncan et al. (2025) |
| Environmental and Gene-Environment Interactions | 15–40% risk from exposures; winter birth OR elevated in Northern Hemisphere | Adults with schizophrenia (matches question population) | Positive (increased risk) | Strong (consistent across multiple studies with reasonable designs) | Robinson & Bergen (2021), Coury et al. (2023), Schmitt et al. (2022) |
| Neurobiological Mechanisms | Synaptic overpruning reduces density; E/I imbalance via GABA/glutamate variants | Patients with schizophrenia (matches question population) | Positive (pathophysiological link) | Moderate (generally consistent but mixed measures) | Howes & Shatalina (2022), Sonnenschein et al. (2020), Kraguljac et al. (2021) |
| Pharmacological Treatments | Ulotaront PANSS −22.6 (95% CI −25.6, −19.6); lumateperone EPS 3.0%; cariprazine augmentation PANSS −43.4% | Adults with schizophrenia, including treatment-resistant (matches question population) | Positive (symptom reduction) | Strong (consistent across multiple independent studies with reasonable designs) | Correll et al. (2021), Edinoff et al. (2025), Pappa et al. (2025a), Laszlovszky et al. (2021), Durgam et al. (2020) |
| Psychosocial Interventions | Family g=1.28 functioning; MBI g=0.72 symptoms | Adults with schizophrenia and caregivers (matches question population) | Positive (improvement) | Moderate (generally consistent but limited contexts) | Kim & Park (2023), Hodann-Caudevilla et al. (2020) |
| Comorbid Risks | T2DM OR=2.15 (95% CI 1.83–2.52); higher in females/Europe | Adults with schizophrenia (matches question population) | Positive (increased risk) | Strong (consistent across multiple studies with reasonable designs) | Dong et al. (2024) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis reveals schizophrenia's etiology as a convergence of polygenic risks and environmental insults disrupting neurodevelopmental trajectories, culminating in dopaminergic and E/I imbalances that manifest as core symptoms. Genetic burdens like exon-proximal TREs and neuronal subtype associations explain synaptic vulnerabilities, while environmental factors such as winter birth and adversity amplify these through prenatal circuit perturbations, accounting for a substantial non-heritable risk fraction. This interplay likely drives overpruning and hippocampal-prefrontal dysconnectivity, as evidenced by reduced synaptic density and upstream regulation failures, providing a mechanistic bridge from early insults to adult psychosis. Novel treatments exploit these pathways: ulotaront and lumateperone's TAAR1/5-HT1A and multi-transmitter modulation achieve efficacy at low D2 occupancy (e.g., 40%), minimizing EPS (3.0% incidence) while sustaining PANSS reductions (−22.6 points), unlike D2-heavy agents risking metabolic harms. Cariprazine's D3 preference enhances negative symptom targeting (59.1% subscale reduction), synergizing with clozapine to address resistance via complementary receptor effects. Psychosocial approaches like family interventions bolster functioning (g=1.28) by mitigating caregiver burden, complementing pharmacology. Confidence is highest in pharmacological efficacy, backed by RCTs with consistent effect sizes, reflecting robust designs in diverse adult cohorts; etiological mechanisms are moderately confident, as neuroimaging and genomic syntheses align but lack longitudinal causal tracking. This review uniquely highlights how polygenic scores could personalize risk assessment, revealing patterns like regional T2DM disparities (OR=2.73 in Europe) that individual studies overlook, advancing toward circuit-specific therapies.
4.2 Comparison with Existing Literature and Resolution of Contradictions
Findings align with longstanding dopamine hypotheses, extending them through integrated models where E/I imbalances—via glutamatergic variants—underlie hyperdopaminergia, consistent with prior imaging showing subcortical hyperactivity; this mechanistic consistency strengthens the neurodevelopmental framework, implying resilience in compensatory circuits explains variable onset. Environmental risks echo earlier epidemiology, with winter birth patterns reinforcing infection/nutrition hypotheses, but the synthesis clarifies hemispheric differences, attributing Southern null effects to methodological variations in cohort latitudes rather than biological nullity. Contradictions in gene-environment interactions, where early candidate gene studies underpowered null results while polygenic approaches suggest synergies, likely stem from sample sizes and genomic resolution; smaller, pre-2020 studies lacked GWAS-scale power, whereas recent syntheses resolve this by demonstrating enriched TREs in adversity-exposed families, indicating true interactions obscured by prior designs. For treatments, cariprazine augmentation's mixed outcomes (e.g., 17% discontinuation vs. 83% negative symptom gains) contrast uniform D2 antagonist benefits, potentially reflecting population heterogeneity in treatment resistance—clozapine non-responders with prominent negatives respond better due to D3 modulation, unlike positive-dominant cases showing anxiety exacerbation. Publication bias risk is low for pharmacological themes, given placebo-controlled RCTs, but higher for etiological reviews, where positive associations dominate, possibly from selective reporting of significant risks. Methodological evolution, from narrative to meta-analytic designs post-2020, refines estimates, with pooled ORs for T2DM (2.15) more precise than isolated cohorts, underscoring improved confounding adjustment in recent work.
4.3 Practical Implications
For clinicians, these findings advocate prioritizing novel antipsychotics like lumateperone (42 mg/day) or ulotaront (25–75 mg/day) in adults with acute or stable schizophrenia, particularly those at metabolic risk, as evidenced by reduced weight (−0.3 kg) and T2DM odds mitigation; in treatment-resistant cases (30–70% prevalence), cariprazine augmentation to clozapine targets persistent negatives, benefiting outpatients with apathy/social isolation by improving adherence without exacerbating EPS. Psychosocially, individual family interventions should be integrated for caregivers of community-dwelling adults, reducing relapse under high-burden conditions like urban living. Public health strategies must address environmental risks by enhancing prenatal screening in winter-born Northern Hemisphere populations and adversity-exposed youth, potentially lowering 15–40% attributable risk through targeted interventions like infection prevention. Regulatory implications include reevaluating standards for antipsychotics, favoring low-D2 agents to curb EPS (3.0% vs. 6.3%) and metabolic comorbidities (female OR=2.12), especially since no safe threshold exists for genetic-environmental synergies—implying population-wide genomic counseling rather than reactive pharmacotherapy. These apply to DSM-5-diagnosed adults but not acute pediatric cases, where evidence is insufficient; practitioners should monitor T2DM in European females over long follow-up (>20 years, OR=3.17), tailoring to socioeconomic vulnerabilities.
4.4 Strengths and Limitations
Strengths include the comprehensive database search capturing diverse designs from genomics to trials, enabling thematic synthesis of etiological and treatment advances, with prioritized extracted data ensuring structured analysis. Limitations of included studies encompass reliance on syntheses without primary data in reviews, heterogeneous populations (e.g., treatment-resistant subsets), and preclinical elements partially matching human focus, potentially inflating mechanistic confidence. This review's limitations involve abstract-based screening risking overlooked nuances, no formal meta-regression for heterogeneity (e.g., I²=98.9% in T2DM), and extraction focused on key fields without full-text bias assessment, though qualitative synthesis mitigates this.
5. Gaps and Future Directions
Key gaps include sparse direct evidence on gene-environment interactions, with syntheses calling for larger cohorts using polygenic scores to quantify synergies in prenatal adversity-exposed adults, as current data infer rather than test causality. Longitudinal studies tracking neuronal associations from GWAS to symptom onset are absent, particularly in underrepresented Southern Hemisphere or non-European populations where birth season effects nullify. Mechanistic voids persist in how E/I imbalances translate to cognitive deficits, lacking human stem cell models beyond preclinical IEG upregulation. For treatments, randomized controlled trials (RCTs) of cariprazine-clozapine combinations are needed in diverse treatment-resistant subgroups, with harmonized PANSS endpoints to resolve discontinuation variability (17%). Methodological improvements like personal genetic profiling and circuit-specific neuroimaging would strengthen evidence, addressing proxy reliance in comorbid risks (e.g., T2DM in schizophrenia vs. general psychosis). Targeted research on pediatric-to-adult transitions and sex-specific metabolic trajectories is essential to fill demographic underrepresentation.
6. Conclusion
Research from 2020 to 2025 establishes schizophrenia as arising from polygenic risks like TRE enrichments at synaptic loci, interacting with environmental factors such as winter birth and childhood adversity to disrupt neurodevelopmental circuits, yielding dopamine dysregulation and E/I imbalances that underpin positive, negative, and cognitive symptoms in adults. Novel antipsychotics offer robust alternatives, with ulotaront achieving sustained PANSS reductions of −22.6 (95% CI −25.6, −19.6) at low D2 occupancy, lumateperone limiting EPS to 3.0%, and cariprazine augmentation yielding 43.4% PANSS improvements in resistant cases, complemented by psychosocial gains like g=1.28 in family functioning. These patterns hold for DSM-5-diagnosed adults but draw partially from treatment-resistant subsets, warranting caution in generalizing to early-onset groups. Elevated T2DM risks (OR=2.15; 95% CI 1.83–2.52), higher in females, underscore metabolic vigilance. The most critical unresolved question is the precise timing and magnitude of gene-environment effects, essential for preventive strategies. Understanding these advances could transform schizophrenia management, reducing comorbidity burdens and enabling personalized interventions, ultimately improving quality of life for millions affected worldwide—motivating urgent, integrative research to close mechanistic gaps.
References
Begni, V., Sanson, A., Luoni, A., Sensini, F., Grayson, B., Munni, S., Neill, J. C., & Riva, M. A. (2021). Towards novel treatments for schizophrenia: Molecular and behavioural signatures of the psychotropic agent SEP-363856. International Journal of Molecular Sciences, 22, 4119. https://doi.org/10.3390/ijms22084119
Correll, C. U., Koblan, K. S., Hopkins, S. C., Li, Y., Dworak, H., Goldman, R., & Loebel, A. (2021). Safety and effectiveness of ulotaront (SEP-363856) in schizophrenia: Results of a 6-month, open-label extension study. Schizophrenia, 7, 63. https://doi.org/10.1038/s41537-021-00190-z
Coury, S. M., Lombroso, A., Avila-Quintero, V. J., Taylor, J. H., Flores, J. M., Szejko, N., & Bloch, M. H. (2023). Systematic review and meta-analysis: Season of birth and schizophrenia risk. Schizophrenia Research, 252, 244–252. https://doi.org/10.1016/j.schres.2022.12.016
Darriba, H. B. (2021). Combined use of clozapine and cariprazine in treatment-resistant schizophrenia, is it a good choice? European Psychiatry, 64, S798–S799. https://doi.org/10.1192/j.eurpsy.2021.2111
Dong, K., Wang, S., Qu, C., Zheng, K., & Sun, P. (2024). Schizophrenia and type 2 diabetes risk: A systematic review and meta-analysis. Frontiers in Endocrinology, 15, 1395771. https://doi.org/10.3389/fendo.2024.1395771
Duncan, L. E., Li, T., Salem, M., Li, W.-M., Mortazavi, L., Senturk, H., Shahverdizadeh, N., Vesuna, S., Shen, H., Yoon, J. H., Wang, G., Ballon, J. S., Tan, L., Pruett, B. S., Knutson, B., Deisseroth, K., & Giardino, W. J. (2025). Mapping the cellular etiology of schizophrenia and complex brain phenotypes. Nature Neuroscience, 28, 248–258. https://doi.org/10.1038/s41593-024-01834-w
Durgam, S., Satlin, A., Davis, R. E., Vanover, K. E., Mates, S., & Kane, J. M. (2020). T205. Lumateperone in the treatment of schizophrenia: Evaluation of extrapyramidal and motor symptoms in 4 late-phase clinical trials. Schizophrenia Bulletin, 46, S310. https://doi.org/10.1093/schbul/sbaa029.765
Edinoff, A. N., Wu, N. W., deBoisblanc, C., Feltner, C. O., Norder, M., Tzoneva, V., Kaye, A. M., Cornett, E. M., Kaye, A. D., Viswanath, O., & Urits, I. (2025). Lumateperone for the treatment of schizophrenia. Psychopharmacology Bulletin, 50, 32–59. https://doi.org/10.64719/pb.4372
Hodann-Caudevilla, R. M., Díaz-Silveira, C., Burgos-Julián, F. A., & Germán, M. Á. S. (2020). Mindfulness-based interventions for people with schizophrenia: A systematic review and meta-analysis. International Journal of Environmental Research and Public Health, 17, 4690. https://doi.org/10.3390/ijerph17134690
Howes, O., & Shatalina, E. (2022). Integrating the neurodevelopmental and dopamine hypotheses of schizophrenia and the role of cortical excitation-inhibition balance. Biological Psychiatry, 92, 501–513. https://doi.org/10.1016/j.biopsych.2022.06.017
Kim, S., & Park, S. (2023). Effectiveness of family interventions for patients with schizophrenia: A systematic review and meta-analysis. International Journal of Mental Health Nursing, 32, 1598–1615. https://doi.org/10.1111/inm.13198
Kraguljac, N. V., McDonald, W. M., Widge, A. S., Rodríguez, C. I., Tohen, M., & Nemeroff, C. B. (2021). Neuroimaging biomarkers in schizophrenia. American Journal of Psychiatry, 178, 509–521. https://doi.org/10.1176/appi.ajp.2020.20030340
Laszlovszky, I., Barabássy, Á., & Németh, G. (2021). Cariprazine, a broad-spectrum antipsychotic for the treatment of schizophrenia: Pharmacology, efficacy, and safety. Advances in Therapy, 38, 3652–3673. https://doi.org/10.1007/s12325-021-01797-5
Mojarad, B. A., Engchuan, W., Trost, B., Backstrom, I., Yin, Y., Thiruvahindrapuram, B., Pallotto, L. M., Mitina, A., Khan, M., Pellecchia, G., Haque, B., Guo, K., Heung, T., Costain, G., Scherer, S. W., Marshall, C. R., Pearson, C. E., Bassett, A. S., & Yuen, R. K. C. (2022). Genome-wide tandem repeat expansions contribute to schizophrenia risk. Molecular Psychiatry, 27, 3692–3698. https://doi.org/10.1038/s41380-022-01575-x
Pappa, S., Csehi, R., Caldwell-Dunn, E., Dombi, Z. B., & Hjorth, S. (2025a). Cariprazine and clozapine: A systematic review of a promising antipsychotic combination for treatment-resistant schizophrenia. The International Journal of Neuropsychopharmacology, 28. https://doi.org/10.1093/ijnp/pyaf053
Pappa, S., Dombi, Z. B., Caldwell-Dunn, E., Csehi, R., & Barabássy, Á. (2025b). Cariprazine & clozapine: A systematic review of a promising combination in the management of treatment-resistant schizophrenia. European Psychiatry, 68, S254. https://doi.org/10.1192/j.eurpsy.2025.563
Robinson, N., & Bergen, S. E. (2021). Environmental risk factors for schizophrenia and bipolar disorder and their relationship to genetic risk: Current knowledge and future directions. Frontiers in Genetics, 12, 686666. https://doi.org/10.3389/fgene.2021.686666
Saarinen, M., Mantas, I., Flais, I., Ågren, R., Sahlholm, K., Millan, M. J., & Svenningsson, P. (2022). TAAR1 dependent and independent actions of the potential antipsychotic and dual TAAR1/5-HT1A receptor agonist SEP-363856. Neuropsychopharmacology, 47, 2319–2329. https://doi.org/10.1038/s41386-022-01421-2
Schmitt, A., Falkai, P., & Papiol, S. (2022). Neurodevelopmental disturbances in schizophrenia: Evidence from genetic and environmental factors. Journal of Neural Transmission, 130, 195–205. https://doi.org/10.1007/s00702-022-02567-5
Sonnenschein, S. F., Gomes, F. V., & Grace, A. A. (2020). Dysregulation of midbrain dopamine system and the pathophysiology of schizophrenia. Frontiers in Psychiatry, 11, 613. https://doi.org/10.3389/fpsyt.2020.00613