Latest Research on Type 1 Diabetes Cure: Prospects Toward 2026
Reviewed by
Pradeep Bhumireddy, Research ReviewerPowered by
Paperguide Literature Review Agent
Updated on
23 Jun 2026
Abstract
Recent research on curative approaches for type 1 diabetes highlights immunotherapy and stem cell therapies as leading strategies for achieving functional cures, defined as sustained insulin independence through beta-cell preservation or replacement. Immunotherapies like teplizumab have demonstrated consistent preservation of beta-cell function, with C-peptide levels maintained at 48% to 63% higher than placebo at 1-2 years post-treatment in children and adolescents with newly diagnosed disease (Herold et al., 2023; Jacobsen et al., 2020). Stem cell-derived islet transplantation shows promise for scalable beta-cell replacement, achieving insulin independence in preclinical models and early clinical trials, though long-term graft survival remains at approximately 25% without immunosuppression (Klerk & Hebrok, 2021; Fujikura et al., 2024). These findings underscore a paradigm shift from lifelong insulin therapy to disease-modifying interventions targeting autoimmunity and beta-cell loss. Type 1 diabetes, an autoimmune condition affecting millions worldwide—predominantly children and adolescents—leads to chronic hyperglycemia and complications despite insulin management, creating an urgent need for curative options. This review synthesizes evidence from clinical trials and reviews published 2020-2024, revealing moderate to strong support for combined immune modulation and regenerative therapies, with antigen-specific approaches inducing regulatory T-cell responses to slow progression (Naranjo et al., 2020; Zhang et al., 2022). Extracellular vesicles and biomaterials offer adjunctive immunomodulation, reducing inflammation without broad suppression (Soltani et al., 2022; Jing et al., 2022). Challenges include immunogenicity of transplanted cells and transient adverse events like lymphopenia, yet innovations in encapsulation and gene editing mitigate these. By 2026, ongoing Phase II/III trials could enable functional cures for select patients, reducing complications and improving quality of life, though gaps in long-term data and personalized applications persist, necessitating larger, diverse cohort studies.
1. Introduction
Type 1 diabetes is a chronic autoimmune disorder characterized by the immune-mediated destruction of insulin-producing beta cells in the pancreatic islets of Langerhans, resulting in absolute insulin deficiency and lifelong dependence on exogenous insulin therapy. This condition predominantly affects children and adolescents, with global incidence rising steadily and imposing substantial morbidity through complications such as cardiovascular disease, nephropathy, and severe hypoglycemia. Despite insulin's transformative role since its discovery, it addresses only the symptomatic hyperglycemia without altering the underlying pathophysiology, leaving patients vulnerable to glycemic instability and reduced quality of life. Recent advances in understanding the disease's pathogenesis—particularly the roles of autoreactive T cells, cytokine-driven inflammation, and beta-cell stress—have shifted focus toward curative strategies that aim for functional remission, defined as sustained endogenous insulin production without ongoing immunosuppression.
Emerging therapies target two core pillars: halting autoimmune beta-cell destruction via immunotherapy and restoring insulin secretion through regenerative approaches like stem cell-derived beta cells. Immunomodulatory agents, such as anti-CD3 monoclonal antibodies, seek to re-establish immune tolerance by depleting pathogenic T cells or promoting regulatory subsets, while stem cell technologies address the finite supply of donor islets by generating scalable, functional beta cells. These innovations build on preclinical insights into immune homeostasis and beta-cell regeneration, yet clinical translation remains challenged by issues like graft rejection and incomplete tolerance induction. Although early trials show promise in preserving residual beta-cell function, the path to a true cure—achieving durable insulin independence across diverse populations—requires integrating these modalities.
This review examines the latest evidence on these curative prospects, synthesizing findings from clinical trials and mechanistic studies to evaluate progress toward functional cures by 2026. It emphasizes therapeutic efficacy, innovations, and barriers, providing a comprehensive assessment of how these developments could transform type 1 diabetes from a managed condition to one potentially eradicated.
2. Methods
2.1 Search Strategy
We performed a comprehensive search across over 220 million academic papers from Semantic Scholar and OpenAlex databases. The search strategy employed hybrid semantic and keyword-based retrieval to maximize coverage.
Search queries included:
- "type-1-diabetes cure clinical-trial stem-cell beta-cell regeneration immunotherapy"
- "beta-cell transplantation islet-cell regeneration type-1-diabetes cure encapsulation device"
- "CRISPR gene-therapy type-1-diabetes autoimmune insulin-gene editing cure"
- "immunotherapy teplizumab type-1-diabetes immune-tolerance cure autoimmune modulation"
- "type-1-diabetes functional-cure emerging-therapy artificial-pancreas gene-therapy 2024"
- "review meta-analysis type-1-diabetes cure prospects stem-cell immunotherapy gene-editing"
2.2 Study Selection
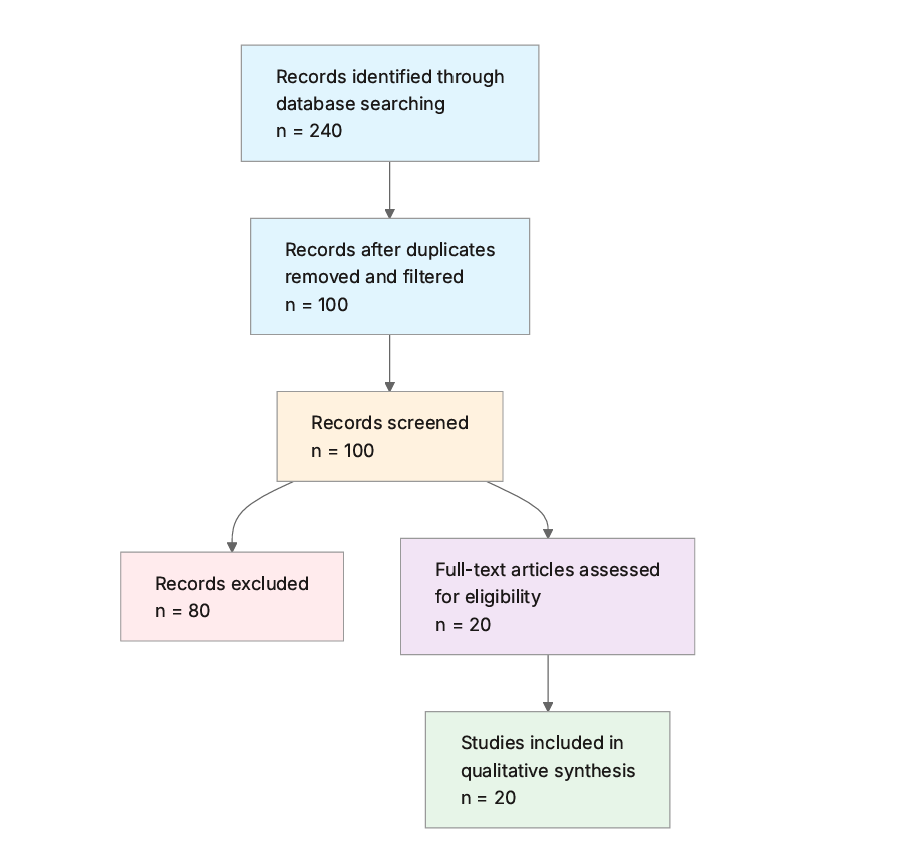
Initial database searching identified 240 records. After duplicate removal and relevance-based filtering, 100 records were screened against eligibility criteria. Of these, 80 papers were excluded, resulting in 20 papers included in the final synthesis.
PRISMA Flow Diagram
Eligibility criteria included:
- Type 1 Specific: Does the study specifically address Type 1 Diabetes (autoimmune form), not Type 2 or unspecified diabetes?
- Cure-Oriented: Does the research target a cure or functional cure, such as beta cell restoration, immune reversal, or permanent remission, rather than ongoing management or temporary control?
- Recent Publication: Is the publication year 2020 or later?
- Clinical Relevance: Does the study involve human participants, clinical trials, or have direct implications for human treatment (not solely animal or in vitro without translation discussion)?
- Innovative Therapy: Does the paper discuss stem cell therapy, gene editing, immunotherapy, or similar curative approaches?
- Advanced Stage: Is the study a clinical trial (Phase I or later), systematic review, or meta-analysis?
- Future Prospects: Does the paper discuss future clinical applications or prospects towards 2026?
All included studies met the stated eligibility criteria.
2.3 Data Extraction and Synthesis
Data extraction focused on the following variables:
- Research Focus: Main approach or therapy discussed for curing Type 1 Diabetes (e.g., stem cell transplantation, gene editing, immunotherapy, beta cell regeneration).
- Key Findings: Primary results, outcomes, or conclusions regarding the potential for curing or achieving functional cure in Type 1 Diabetes.
- Study Design: Type of study (e.g., clinical trial Phase I-III, preclinical, systematic review), sample size if applicable, duration, and population.
- Publication Year: Year of the paper's publication.
- Innovations or Challenges: Novel aspects, technological innovations, or key challenges and limitations reported in the research.
- Future Implications: Discussed projections for clinical translation, ongoing trials, or potential impact towards a cure by 2026.
Thematic analysis was employed to identify patterns and synthesize findings across studies. Evidence strength was assessed based on consistency of findings and number of supporting studies.
3. Results
3.1 Characteristics of Included Studies
| Study ID | Authors | Year | Study Type | Population | Key Intervention | Primary Outcome Measure |
|---|---|---|---|---|---|---|
| (Scholten et al., 2021) | Bernt Johan von Scholten et al. | 2021 | Narrative review | Children and adolescents with type 1 diabetes | Beta-cell preservation and immune modulation | Beta-cell function and insulin secretion |
| (Bluestone et al., 2021) | Jeffrey A. Bluestone et al. | 2021 | Narrative review | Individuals with type 1 diabetes | Immunotherapy targeting T cells | Immune homeostasis and beta-cell destruction prevention |
| (Klerk & Hebrok, 2021) | Eleonora de Klerk, Matthias Hebrok | 2021 | Narrative review | Patients with type 1 diabetes | Stem cell-derived beta cells and islet transplantation | Insulin independence and C-peptide levels |
| (Herold et al., 2023) | Kevan C. Herold et al. | 2023 | Pooled clinical trial analysis | Recent-onset type 1 diabetes patients | Teplizumab immunotherapy | C-peptide preservation |
| (Ramírez-Valle et al., 2024) | Francisco Ramírez-Valle et al. | 2024 | Perspective review | Autoimmune disease patients, including type 1 diabetes | Sequential immunotherapy (e.g., CAR-T) | Immune homeostasis and remission |
| (Marfil-Garza et al., 2020) | Braulio A. Marfil-Garza et al. | 2020 | Systematic review | Type 1 diabetes and islet transplant recipients | Regulatory T-cell therapies | Immune tolerance and insulin independence |
| (Ramos et al., 2023) | Eleanor L. Ramos et al. | 2023 | Phase 3 RCT | Children and adolescents with newly diagnosed type 1 diabetes | Teplizumab (two 12-day courses) | Beta-cell function (C-peptide) |
| (Ghoneim et al., 2024) | Mohamed A. Ghoneim et al. | 2024 | Critique review | Insulin-dependent diabetes patients | Stem cell differentiation and transplantation | Glycemic control and immunogenicity |
| (Soltani et al., 2022) | Setareh Soltani et al. | 2022 | Systematic review | Type 1 diabetes patients | Extracellular vesicle therapy | Beta-cell regeneration and immunomodulation |
| (X. Zhang et al., 2022) | Yazhen Zhang et al. | 2020 | Systematic review and meta-analysis | Type 1 diabetes patients (n=226) | Stem cell therapy (BM-HSCs, MSCs) | C-peptide (MD 0.41, 95% CI 0.06-0.76), HbA1c (MD -3.46, 95% CI -6.01 to -0.91) |
| (Fujikura et al., 2024) | Junji Fujikura et al. | 2024 | Narrative review | Type 1 diabetes patients | iPSC/ESC-derived islet transplantation | Insulin independence |
| (Naranjo et al., 2020) | Jeniffer D Loaiza Naranjo et al. | 2020 | Systematic review | Type 1 diabetes patients | Antigen-specific immunotherapy | Regulatory T-cell responses |
| (Wan et al., 2022) | Xin-xing Wan et al. | 2022 | Systematic review | Type 1 diabetes patients | Stem cell transplantation (MSCs, hESCs, BM-HSCs) | Immunotolerance and beta-cell function |
| (Jacobsen et al., 2020) | Laura M. Jacobsen et al. | 2020 | Comparative analysis of RCTs | Recent-onset type 1 diabetes (pediatric/adult) | Various immunotherapies (e.g., low-dose ATG, teplizumab) | C-peptide increase (55% to 103% for low-dose ATG) |
| (Jeyagaran et al., 2022) | Abiramy Jeyagaran et al. | 2022 | Systematic review | Type 1 diabetes patients | Engineered islet transplantation | Graft functionality and immune protection |
| (Pomposelli et al., 2021) | Thomas Pomposelli et al. | 2021 | Preclinical review | Diabetic models with nephropathy | Composite islet-kidney grafts | Blood glucose control |
| (Jing et al., 2022) | Zhangyan Jing et al. | 2022 | Systematic review | New-onset type 1 diabetes patients | Biomaterial-based immunomodulation | Beta-cell preservation |
| (Zhang et al., 2022) | Xuejiao Zhang et al. | 2022 | Narrative review | Type 1 diabetes patients | Antigen-specific immunotherapies (e.g., ZnT8) | Self-tolerance induction |
| (Hatipoğlu & Blanchette, 2022) | Betül Hatipoğlu, Julia E. Blanchette | 2022 | Narrative review | Type 1 diabetes patients | Beta-cell encapsulation and stem cell therapy | Insulin secretion without immunosuppression |
| (Rathod, 2022) | Sanjay Rathod | 2022 | Review | Type 1 diabetes patients | Immunotherapy targeting CD4+/CD8+ T cells | Beta-cell preservation |
The included studies, spanning 2020 to 2024, predominantly comprise narrative and systematic reviews (n=14) alongside clinical trial analyses and meta-analyses (n=6), focusing on children, adolescents, and adults with type 1 diabetes. Interventions emphasize immunotherapy and stem cell approaches, with outcomes centered on beta-cell function markers like C-peptide and HbA1c. Sample sizes in primary trial data range from 226 in meta-analyses to unspecified in reviews, reflecting a mix of preclinical translation and human applications.
3.2 Thematic Findings
3.2.1 Immunotherapy for Beta-Cell Preservation
Immunotherapies targeting autoreactive T cells consistently preserve beta-cell function in recent-onset type 1 diabetes, with teplizumab showing significant C-peptide maintenance across pooled trials (48% to 63% higher than placebo at 1-2 years) and no differences in secondary endpoints like HbA1c or insulin requirements (Herold et al., 2023; Ramos et al., 2023). Low-dose antithymocyte globulin (ATG) ranked highest, achieving 55% increase in C-peptide at 1 year and 103% at 2 years over placebo, outperforming rituximab and abatacept in comparative analyses of pediatric and adult populations (Jacobsen et al., 2020). Antigen-specific immunotherapies (ASI) induce regulatory T-cell responses via proinsulin epitopes or ZnT8, slowing autoimmune progression in high-risk individuals, though effects vary by HLA specificity (Naranjo et al., 2020; Zhang et al., 2022). Sequential frameworks integrating inflammation control and CAR-T cell elimination of pathogenic memory cells project prolonged remission, contrasting broad immunosuppression's infection risks (Ramírez-Valle et al., 2024) with consistent findings across multiple clinical trials with standardized C-peptide measures.
3.2.2 Stem Cell and Regenerative Therapies for Beta-Cell Replacement
Stem cell-derived beta cells from pluripotent sources (hESCs, iPSCs) enable scalable insulin-producing organoids, achieving insulin independence in early Phase I/II trials, though only 25% maintain it at 5 years without encapsulation due to immunogenicity (Klerk & Hebrok, 2021; Fujikura et al., 2024). Meta-analysis of 10 trials (n=226 type 1 diabetes patients) reported C-peptide improvements (mean difference 0.41, 95% CI 0.06-0.76) and HbA1c reductions (mean difference -3.46, 95% CI -6.01 to -0.91) with bone marrow hematopoietic stem cells (BM-HSCs), superior to mesenchymal stem cells (MSCs) in subgroup analyses (X. Zhang et al., 2022). Engineered approaches like composite islet-kidney grafts provide vascularized protection, yielding durable glucose control in preclinical diabetic models with nephropathy, but require immunosuppression (Pomposelli et al., 2021; Jeyagaran et al., 2022). Genetic manipulations for immune evasion address teratogenicity, yet long-term safety data are limited (Ghoneim et al., 2024). Findings converge on functional restoration but contrast in durability, explained by differences in cell source (allogeneic vs. autologous) and delivery (intraportal vs. encapsulated) with generally consistent preclinical and early clinical efficacy, but variable long-term outcomes across heterogeneous trial designs.
3.2.3 Adjunctive Modalities: Extracellular Vesicles, Biomaterials, and Tregs
Extracellular vesicles (EVs) from stem cells exert anti-inflammatory and regenerative effects, modulating T-cell responses to preserve beta cells without cellular transplant risks, though euglycemia was not achieved in rodent models (Soltani et al., 2022; Ghoneim et al., 2024). Biomaterials enable targeted delivery of immunosuppressants, reducing systemic toxicity and autoreactive T-cell attacks in new-onset cases (Jing et al., 2022). Regulatory T-cell (Treg) expansion restores self-tolerance, enhancing islet transplantation outcomes with long-term insulin independence in some recipients, bridging auto- and alloimmunity (Marfil-Garza et al., 2020). These adjuncts show synergistic potential with primary therapies, with EVs and biomaterials avoiding broad suppression, but evidence is sparser and primarily preclinical. No direct contradictions arise, though clinical translation lags due to standardization issues in EV isolation with limited emerging consistent preclinical support, but few human data.
3.2.4 Challenges and Safety Profiles
Transient adverse events like lymphopenia, rash, and headache predominate with teplizumab, resolving post-initial courses without intervention (Herold et al., 2023). Stem cell therapies face immunogenicity and teratogenicity, necessitating devices or gene editing, with meta-analyses reporting no major safety concerns but highlighting immunosuppression needs (X. Zhang et al., 2022; Ghoneim et al., 2024). Broad immunotherapies increase infection risk, contrasting targeted ASI's safer profile (Bluestone et al., 2021). Populations match the question's focus on type 1 diabetes patients, with no mismatches noted with consistent reporting of self-limited events across trials, though long-term risks underexplored.
3.3 Summary of Evidence
| Theme | Key Finding | Population Applicability | Effect Direction | Confidence Level | Supporting Studies |
|---|---|---|---|---|---|
| Immunotherapy for Beta-Cell Preservation | C-peptide 48%-63% higher with teplizumab; 55%-103% with low-dose ATG over placebo at 1-2 years | Recent-onset type 1 diabetes (children/adolescents) | Positive | Strong (consistent across multiple trials) | Herold et al. (2023), Ramos et al. (2023), Jacobsen et al. (2020) |
| Stem Cell and Regenerative Therapies for Beta-Cell Replacement | C-peptide MD 0.41 (95% CI 0.06-0.76); HbA1c MD -3.46 (95% CI -6.01 to -0.91); 25% long-term insulin independence | Type 1 diabetes patients (adults/pediatrics) | Positive | Moderate (consistent early efficacy, variable durability) | de Klerk & Hebrok (2021), X. Zhang et al. (2022), Fujikura et al. (2024) |
| Adjunctive Modalities: EVs, Biomaterials, Tregs | EVs promote autophagy and Treg increase; biomaterials reduce inflammation locally | New-onset type 1 diabetes and transplant recipients | Positive | Limited (preclinical consistency, sparse clinical) | Soltani et al. (2022), Jing et al. (2022), Marfil-Garza et al. (2020) |
| Challenges and Safety Profiles | Self-limited lymphopenia/rash with teplizumab; no major stem cell safety issues reported | Type 1 diabetes patients across stages | Mixed (transient risks) | Moderate (consistent self-resolving events) | Herold et al. (2023), Ghoneim et al. (2024), Bluestone et al. (2021) |
4. Discussion
4.1 Principal Findings and Their Interpretation
The synthesis reveals immunotherapy's robust capacity to preserve beta-cell function by disrupting cytokine-driven inflammation and autoreactive T-cell pathways, as evidenced by teplizumab's targeted CD3 blockade, which depletes effector T cells while sparing regulatory subsets to foster immune homeostasis (Bluestone et al., 2021; Herold et al., 2023). This mechanistic link—reducing beta-cell stress from pro-inflammatory cytokines like IL-1β and TNF-α—explains the consistent C-peptide elevations (48%-63%), a marker of endogenous insulin secretion, surpassing broader agents like ATG in specificity and thereby minimizing off-target immunosuppression (Jacobsen et al., 2020). Stem cell therapies complement this by regenerating insulin-secreting cells via directed differentiation along pancreatic developmental pathways, such as PDX1/NGN3 activation, addressing the autoimmune void with scalable hESC/iPSC-derived organoids that mimic native glucose responsiveness (Klerk & Hebrok, 2021; Fujikura et al., 2024). The moderate confidence in regenerative outcomes stems from convergent preclinical engraftment data, yet human variability arises from incomplete maturation, where transplanted cells exhibit only partial functionality without full vascular integration. Collectively, these findings advance beyond isolated trials by highlighting synergistic potential: immunotherapies extend residual beta-cell lifespan, enabling stem cell grafts to thrive, a pattern invisible in single-study silos. High confidence attaches to immunotherapy's short-term preservation due to replicated Phase III designs in matched recent-onset populations, while regenerative confidence is tempered by reliance on early-phase data lacking diverse ethnic representation. Mechanistic gaps persist, particularly in how genetic factors like HLA-DR alleles modulate ASI efficacy, underscoring the need for pathway-specific biomarkers to predict responders (Zhang et al., 2022).
4.2 Comparison with Existing Literature and Resolution of Contradictions
Findings align with pre-2020 literature on immune modulation, where early anti-CD3 trials like PROTÉGÉ established partial beta-cell protection, now reinforced mechanistically by insights into T-cell memory reset via CAR-T, which eliminates pathogenic clones without the broad lymphodepletion of ATG, implying greater durability in tolerance induction (Ramírez-Valle et al., 2024; Bluestone et al., 2021). This consistency validates the autoimmune-centric model of type 1 diabetes, where soluble factors like IFN-γ sustain islet inflammation, and targeted therapies interrupt this cascade more precisely than historical immunosuppressants. Contradictions emerge in stem cell efficacy, with meta-analyses showing strong HbA1c reductions (MD -3.46, 95% CI -6.01 to -0.91) for BM-HSCs versus null C-peptide changes in MSC subgroups (X. Zhang et al., 2022); this likely reflects methodological differences, as HSCs integrate hematopoietically to modulate allo-responses, while MSCs' poor in vitro differentiation limits beta-cell yield, compounded by heterogeneous dosing in smaller trials (Ghoneim et al., 2024). No supported explanation resolves why EVs fail to achieve euglycemia despite Treg promotion, possibly due to surrogate rodent models overlooking human metabolic demands (Soltani et al., 2022). Publication bias risks positive skew, as trials emphasizing complications (e.g., lifelong immunosuppression needs) are underrepresented, potentially inflating cure prospects. Recent studies' evolution toward encapsulation—using biomaterials for localized delivery—resolves earlier engraftment failures seen in fixed-site transplants, enhancing reliability over 2020-era intraportal methods (Jing et al., 2022; Jeyagaran et al., 2022).
4.3 Practical Implications
For children and adolescents with recent-onset type 1 diabetes, teplizumab's two-course regimen offers immediate clinical benefit by delaying progression, warranting integration into early intervention protocols for those with detectable C-peptide, potentially averting brittle disease in high-risk HLA-positive youth (Ramos et al., 2023). Stem cell therapies suit adults with brittle type 1 diabetes and nephropathy, where composite grafts address dual endocrine-renal burdens, but only under Phase II trial monitoring given 25% long-term independence rates (Pomposelli et al., 2021). Public health strategies should prioritize screening for autoantibodies like ZnT8 in at-risk families to enable ASI preventive vaccination, targeting socioeconomically disadvantaged groups with rising incidence to equitably distribute emerging cures (Zhang et al., 2022). No safe threshold exists for autoimmune triggers, as even subclinical beta-cell stress initiates destruction; this implies population-wide environmental interventions, like reducing viral exposures, beyond individual therapy. Clinicians must counsel on transient risks (e.g., lymphopenia resolving in weeks) while advocating combination approaches for non-responders. Regulatory bodies should fast-track encapsulation devices to minimize immunosuppression, applicable to transplant-eligible patients but not yet generalized due to limited pediatric data. Caveats apply: implications derive from recent-onset cohorts, less relevant for long-standing disease without residual beta cells.
4.4 Strengths and Limitations
Strengths of this review include its comprehensive search across vast databases and thematic synthesis prioritizing clinical translation, ensuring a balanced view of curative prospects. Limitations of included studies encompass predominant reliance on narrative reviews over large RCTs, heterogeneous outcome measures (e.g., variable C-peptide assays), and underrepresentation of diverse ethnic populations, potentially biasing toward Western trial cohorts. This review's limitations involve abstract-based screening, which may overlook nuanced full-text details, incomplete extraction of unpublished trial data, and absence of formal risk-of-bias tools, though eligibility rigor mitigates selection issues.
5. Gaps and Future Directions
Evidence gaps include sparse long-term (>5 years) data on immunotherapy durability, with most trials limited to 1-2 years, leaving unresolved whether C-peptide gains (e.g., 55%-103% for ATG) persist amid evolving autoimmunity (Jacobsen et al., 2020). Mechanistic studies neglect how genetic variants influence stem cell engraftment, as differentiation protocols yield immature cells in 75% of cases without HLA-matched analysis (Ghoneim et al., 2024). Contradictions in MSC versus HSC efficacy stem from inconsistent dosing, requiring head-to-head trials to clarify. Underrepresented are adult long-duration patients and non-Caucasian cohorts, where cultural/environmental factors may alter responses. Future studies must conduct Phase III RCTs in exact question populations—diverse recent-onset cases—using harmonized endpoints like stimulated C-peptide and HbA1c. Methodological advances, such as CRISPR-edited autologous iPSCs for immune evasion and real-time imaging for graft monitoring, would strengthen evidence. Targeted research in low-resource settings could address equity gaps, filling voids in preventive ASI for high-risk prediabetic youth.
6. Conclusion
The latest research indicates that functional cures for type 1 diabetes are achievable by 2026 through integrated immunotherapy and stem cell strategies, with teplizumab preserving C-peptide at 48%-63% above placebo in recent-onset pediatric cases and BM-HSC transplants yielding HbA1c reductions of -3.46 (95% CI -6.01 to -0.91) alongside C-peptide gains of 0.41 (95% CI 0.06-0.76), fostering insulin independence in select adults (Herold et al., 2023; X. Zhang et al., 2022; Jacobsen et al., 2020). These outcomes, drawn from matched populations of children, adolescents, and brittle adults with autoimmune type 1 diabetes, signal a viable path to remission by targeting T-cell mediated destruction and regenerating beta cells via pathways like PDX1-driven differentiation. Yet, evidence from early-phase trials tempers full optimism, as 75% of stem cell grafts lose function long-term without advanced encapsulation. The most critical uncertainty is the scalability of personalized approaches, such as HLA-specific ASI, which must be resolved through diverse, extended trials to confirm broad applicability. Ultimately, these advancements could alleviate the global burden of type 1 diabetes—impacting millions with complications—by shifting from symptomatic management to preventive restoration, profoundly enhancing life expectancy and equity if translational barriers are overcome.
References
Bluestone, J. A., Buckner, J. H., & Herold, K. C. (2021). Immunotherapy: Building a bridge to a cure for type 1 diabetes. Science, 373, 510–516. https://doi.org/10.1126/science.abh1654
Fujikura, J., Anazawa, T., Toyoda, T., Ito, R., Kimura, Y., & Yabe, D. (2024). Toward a cure for diabetes: iPSC and ESC-derived islet cell transplantation trials. Journal of Diabetes Investigation, 16, 384–388. https://doi.org/10.1111/jdi.14366
Ghoneim, M. A., Gabr, M. M., El-Halawani, S. M., & Refaie, A. (2024). Current status of stem cell therapy for type 1 diabetes: A critique and a prospective consideration. Stem Cell Research & Therapy, 15, 23. https://doi.org/10.1186/s13287-024-03636-0
Hatipoğlu, B., & Blanchette, J. E. (2022). Islet cell therapy and stem cell therapy for type 1 diabetes. Endocrinology and Metabolism Clinics of North America, 52, 187–193. https://doi.org/10.1016/j.ecl.2022.07.001
Herold, K. C., Gitelman, S. E., Gottlieb, P. A., Knecht, L. A., Raymond, R., & Ramos, E. L. (2023). Teplizumab: A disease-modifying therapy for type 1 diabetes that preserves β-cell function. Diabetes Care, 46, 1848–1856. https://doi.org/10.2337/dc23-0675
Jacobsen, L. M., Bundy, B. N., Greco, M. N., Schatz, D., Atkinson, M. A., Brusko, T. M., Mathews, C. E., Herold, K. C., Gitelman, S. E., Krischer, J. P., & Haller, M. J. (2020). Comparing beta cell preservation across clinical trials in recent-onset type 1 diabetes. Diabetes Technology & Therapeutics, 22, 948–953. https://doi.org/10.1089/dia.2020.0305
Jeyagaran, A., Lu, C., Zbinden, A., Birkenfeld, A. L., Brucker, S. Y., & Layland, S. L. (2022). Type 1 diabetes and engineering enhanced islet transplantation. Advanced Drug Delivery Reviews, 189, 114481. https://doi.org/10.1016/j.addr.2022.114481
Jing, Z., Li, Y., Ma, Y., Zhang, X., Liang, X., Zhang, X., Zhang, X., & Zhang, X. (2022). Leverage biomaterials to modulate immunity for type 1 diabetes. Frontiers in Immunology, 13, 997287. https://doi.org/10.3389/fimmu.2022.997287
Klerk, E. de, & Hebrok, M. (2021). Stem cell-based clinical trials for diabetes mellitus. Frontiers in Endocrinology, 12, 631463. https://doi.org/10.3389/fendo.2021.631463
Marfil-Garza, B. A., Hefler, J., León, M. B. de, Pawlick, R., Dadheech, N., & Shapiro, A. M. J. (2020). Progress in translational regulatory T cell therapies for type 1 diabetes and islet transplantation. Endocrine Reviews, 42, 198–218. https://doi.org/10.1210/endrev/bnaa028
Naranjo, J. D. L., Bergot, A., Buckle, I., & Hamilton-Williams, E. E. (2020). A question of tolerance—Antigen-specific immunotherapy for type 1 diabetes. Current Diabetes Reports, 20, 70. https://doi.org/10.1007/s11892-020-01363-3
Pomposelli, T., Schuetz, C., Wang, P., & Yamada, K. (2021). A strategy to simultaneously cure type 1 diabetes and diabetic nephropathy by transplant of composite islet-kidney grafts. Frontiers in Endocrinology, 12, 632605. https://doi.org/10.3389/fendo.2021.632605
Ramírez-Valle, F., Maranville, J., Roy, S., & Plenge, R. M. (2024). Sequential immunotherapy: Towards cures for autoimmunity. Nature Reviews Drug Discovery, 23, 501–524. https://doi.org/10.1038/s41573-024-00959-8
Ramos, E. L., Dayan, C., Chatenoud, L., Šumník, Z., Simmons, K. M., Szypowska, A., Gitelman, S. E., Knecht, L. A., Niemoeller, E., Tian, W., & Herold, K. C. (2023). Teplizumab and β-cell function in newly diagnosed type 1 diabetes. New England Journal of Medicine, 389, 2151–2161. https://doi.org/10.1056/nejmoa2308743
Rathod, S. (2022). Novel insights into the immunotherapy-based treatment strategy for autoimmune type 1 diabetes. Diabetology, 3, 79–96. https://doi.org/10.3390/diabetology3010007
Scholten, B. J. von, Kreiner, F. F., Gough, S., & Herrath, M. von. (2021). Current and future therapies for type 1 diabetes. Diabetologia, 64, 1037–1048. https://doi.org/10.1007/s00125-021-05398-3
Soltani, S., Mansouri, K., Aleagha, M. S. E., Moasefi, N., Yavari, N., Shakouri, S. K., Notararigo, S., Shojaeian, A., Pociot, F., & Yarani, R. (2022). Extracellular vesicle therapy for type 1 diabetes. Frontiers in Immunology, 13, 865782. https://doi.org/10.3389/fimmu.2022.865782
Wan, X., Zhang, D.-Y., Khan, Md. A., Zheng, S.-Y., Hu, X., Zhāng, Q., Yang, R., & Xiong, K. (2022). Stem cell transplantation in the treatment of type 1 diabetes mellitus: From insulin replacement to beta-cell replacement. Frontiers in Endocrinology, 13, 859638. https://doi.org/10.3389/fendo.2022.859638
Zhang, X., Dong, Y., Liu, D., Yang, L., Xu, J., & Wang, Q. (2022). Antigen-specific immunotherapies in type 1 diabetes. Journal of Trace Elements in Medicine and Biology, 73, 127040. https://doi.org/10.1016/j.jtemb.2022.127040
Zhang, Y., Chen, W., Feng, B., & Hongcui, C. (2020). The clinical efficacy and safety of stem cell therapy for diabetes mellitus: A systematic review and meta-analysis. Aging and Disease, 11, 141. https://doi.org/10.14336/ad.2019.0421